Table 1
Most common comorbidities in children with sepsis in non-resource-limited settings
Sepsis arises when the body is invaded by an infection, prompting the immune system to fight it.
In response, the immune system becomes hyperactive and targets the body’s organs and tissues. This can result in harm to vital organs such as the kidneys, lungs, brain, and heart, potentially leading to fatal consequences. The best chance of getting better from sepsis is early intervention.
Table 1
Most common comorbidities in children with sepsis in non-resource-limited settings
Table 2
Most common sites of infection and pathogens in sepsisª
Background
The most common pathogens affecting previously healthy children were Staphylococcus aureus (9.4%), streptococcal species (7.9%), and Escherichia coli (7.1%), whereas the most common pathogens in children with chronic diseases were S. aureus (11%), Candida (9.8%), and Pseudomonas (8.1%). More than one-third of children with sepsis do not have an identifiable pathogen. This may be attributed to sepsis being caused by viral aetiologies or because of the limits in detection of bacterial pathogens, particularly if the volume inoculated into blood cultures is low or if the pathogens are fastidious or have specific growth requirements.
Definition of Sepsis
We refer to sepsis as sepsis-associated organ dysfunction and septic shock as sepsis with cardiovascular dysfunction (including hypotension, need for treatment with vasoactive agents, or impaired perfusion). Based on survey data, most paediatric clinicians used sepsis to refer to infection with life-threatening organ dysfunction, which differed from prior paediatric sepsis criteria that used systemic inflammatory response syndrome (SIRS) criteria, which have poor predictive properties, and included the redundant term, severe sepsis.
The Society of Critical Care Medicine (SCCM) task force recommends that sepsis in children be identified by a Phoenix Sepsis Score of at least 2 points in children with suspected infection, which indicates potentially life-threatening dysfunction of the respiratory, cardiovascular, coagulation, and/or neurological systems. Children with a Phoenix Sepsis Score of at least 2 points had in-hospital mortality of 7.1% in higher-resource settings and 28.5% in lower-resource settings, more than 8 times that of children with suspected infection not meeting these criteria.
Mortality was higher in children who had organ dysfunction in at least 1 of 4—respiratory, cardiovascular, coagulation, and/or neurological—organ systems that was not the primary site of infection. Septic shock was defined as children with sepsis who had cardiovascular dysfunction, indicated by at least 1 cardiovascular point in the Phoenix Sepsis Score, which included severe hypotension for age, blood lactate exceeding 5 mmol/L, or need for vasoactive medication. Children with septic shock had an in-hospital mortality rate of 10.8% and 33.5% in higher- and lower-resource settings, respectively.
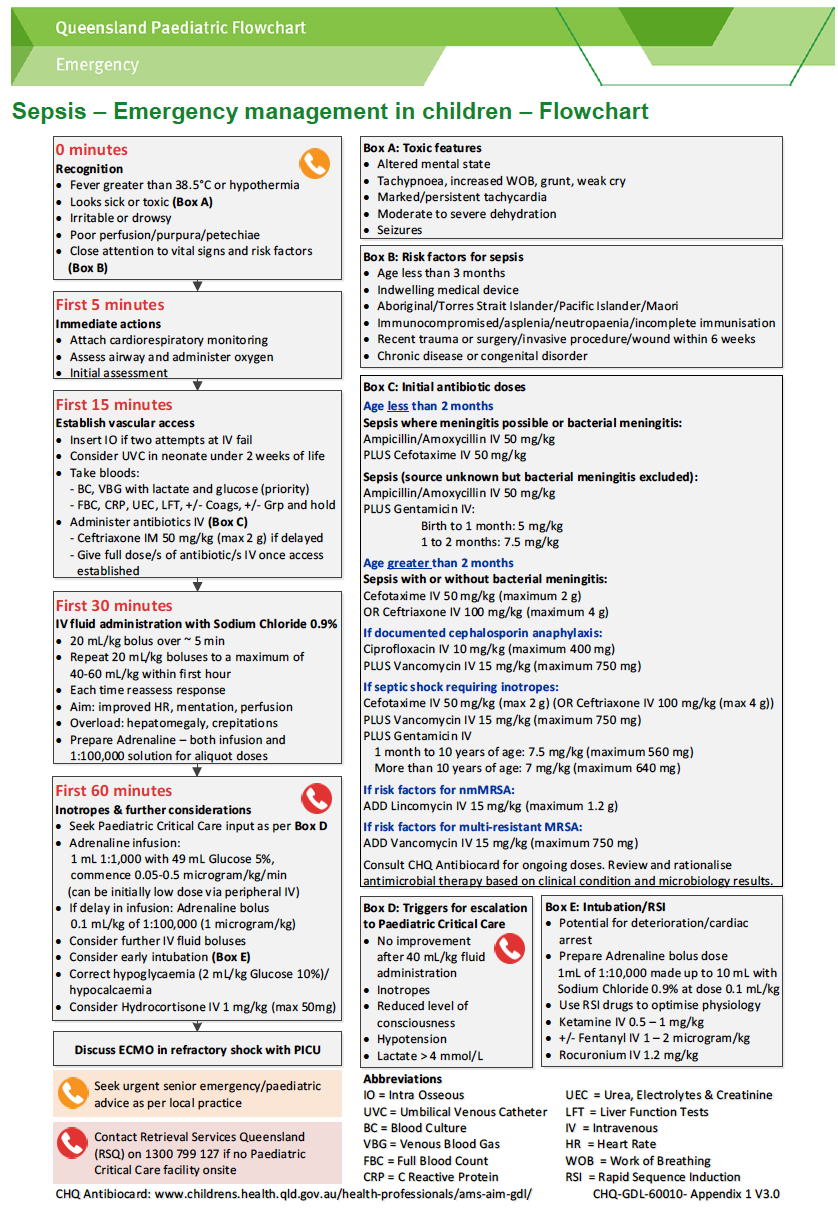
Treatment tool: use the Paediatric Sepsis Pathway (as per CHQ guidelines)
Clinical Guidelines and Tools for Sepsis
Recognition and Emergency Management in Children
Initial Resuscitation Algorithm for Children
Sepsis Pathway Form
Sepsis Flow Chart
Recognition and Emergency Management in children HQ Guideline
This guideline is intended as a guide and provided for the PARIS on Country project during the course of the study period. The information has been prepared using a multidisciplinary approach with reference to the best information and evidence available at the time of preparation. This guideline is based of the Children’s Health Queensland Guideline which can be viewed below.
The guideline is not a substitute for clinical judgement, knowledge and expertise, or medical advice. Variation from the guideline, taking into account individual circumstances may be appropriate.
This guideline does not address all elements of standard practice and accepts that individual clinicians are responsible for:
{kind=link}