- Level ≥4 CSCF facility consultation MUST be sought within 2 hours of HFNC therapy treatment commencing.
- The level ≥4 CSCF facility to your HHS facility consultation should occur at the Senior Medical Officer (SMO) level from both facilities.
- Referring clinician to contact their relevant level ≥4 CSCF facility for consultation – this should be Senior Medical Officer (SMO) level referral at both facilities.
- If a retrieval is clearly required in the first instance contact RSQ (1 300 799 127) to link all relevant parties together including:
- referring SMO from remote hospital
- local level ≥4 CSCF facility
- relevant local Intensive Care Specialist – dependent on the patient’s condition
Remote Management of
High Flow Nasal Cannula therapy in paediatric patients
This procedure describes the processes for the safe and effective use of High Flow Nasal Cannula (HFNC) therapy in children with acute respiratory illnesses. The aim is to support decision making in relation to HFNC therapy initiation, continuation, weaning and escalation of concerns.
Introduction and Aims of HFNC therapy
Scope
The scope of this guideline applies to all participating hospitals in four Hospital and Health Services (HHS) who are performing the PARIS on Country study and providing care to children less than 5 years of age with respiratory illnesses.
This includes the following staff:
• Permanent, temporary and casual employees
• Visiting medical officers, other partners, contractors, consultants, students, trainees and volunteers
• Competent clinicians caring for children receiving HFNC therapy for an acute illness outside of the Intensive Care Unit (ICU) setting.
The hospitals within each HHS include the following – noting the commencement for each site is staggered across 18 months according to their specified randomisation date.
Participating hospitals include:
• North-West HHS – Mt Isa Hospital, Cloncurry, Normanton and Mornington Island hospitals
• Cairns and Hinterland HHS – Atherton, Innisfail, Mareeba, Mossman and Tully hospitals
• Townsville HHS – Ingham, Charters Towers, Ayr hospitals and the Joyce Palmer Health Service, Palm Island.
• Torres and Cape HHS – Weipa, Cooktown, Bamaga and Thursday Island hospitals
Definition of HFNC therapy
HFNC therapy provides non-invasive respiratory support via a warmed, humidified continuous flow of gas that matches the inspiratory flow of the spontaneously breathing infant or child. It creates breath and flow dependent pressure, making inspiration easier and promoting slow, deep breathing on expiration, thereby increasing alveolar ventilation. HFNC therapy pressure is dynamic, not set and not constant. The level of pressure changes through the breath cycle and is dependent on the size of cannula prongs, breathing rate, mouth opened or closes (ie. pressure fluctuates). Oxygen therapy can be added into the flow as an adjunct to HFNC therapy. Inspired oxygen is prescribed as a percentage and titrated to maintain saturations greater than or equal to 90%.
Aims of HFNC therapy
- Improve ventilation and gas exchange (through airflow which flushes the nasopharyngeal dead space and opens distal airways and alveoli)
- Decrease secretion viscosity and mucous membrane drying, improve mucociliary transport, and improve lung compliance (through heated, humidified gas delivery)
- Reduce work of breathing (through all the above)
NOTE : In the acutely unwell child, initial resuscitative measures should be undertaken, and high flow applied thereafter.
Clinical indications, Contraindications, Complications for HFNC therapy
Clinical indications
The prevention of, or relief from moderate to severe respiratory distress, and/or hypoxaemia (SpO²<90%) due to diseases such as:
- bronchiolitis
- pneumonia
- chronic lung disease
- congestive heart failure
- reactive airways disease (pre-school wheeze)
- acute lower respiratory tract infection where the use of standard oxygen therapy has been unsuccessful.
Contraindications for HFNC therapy
- Critically ill child with immediate need for NIV/intubation
- Apnoeas requiring NIV/intubation
- Decreased level of consciousness (GCS ≤8)
- Pneumothorax
- Foreign body aspiration- suspected or confirmed
- Upper airway obstruction:
- Epiglottitis
- Croup
- Cyanotic congenital heart disease (unless in consultation with paediatric cardiologist)
- Choanal atresia (congenital narrowing of the back of the nasal cavity)
- Craniofacial malformations or injuries
- Severe Oro-pharyngeal mucositis
- Trans-oesophageal fistula pre- and post-op
Complications from HFNC therapy
- Gastric distension
- Pressure areas (facial / nasal)
- Blocked cannula due to secretions
- Pneumothorax
Referral & Consultation
- A patient must be accepted at an SMO level at the receiving facility.
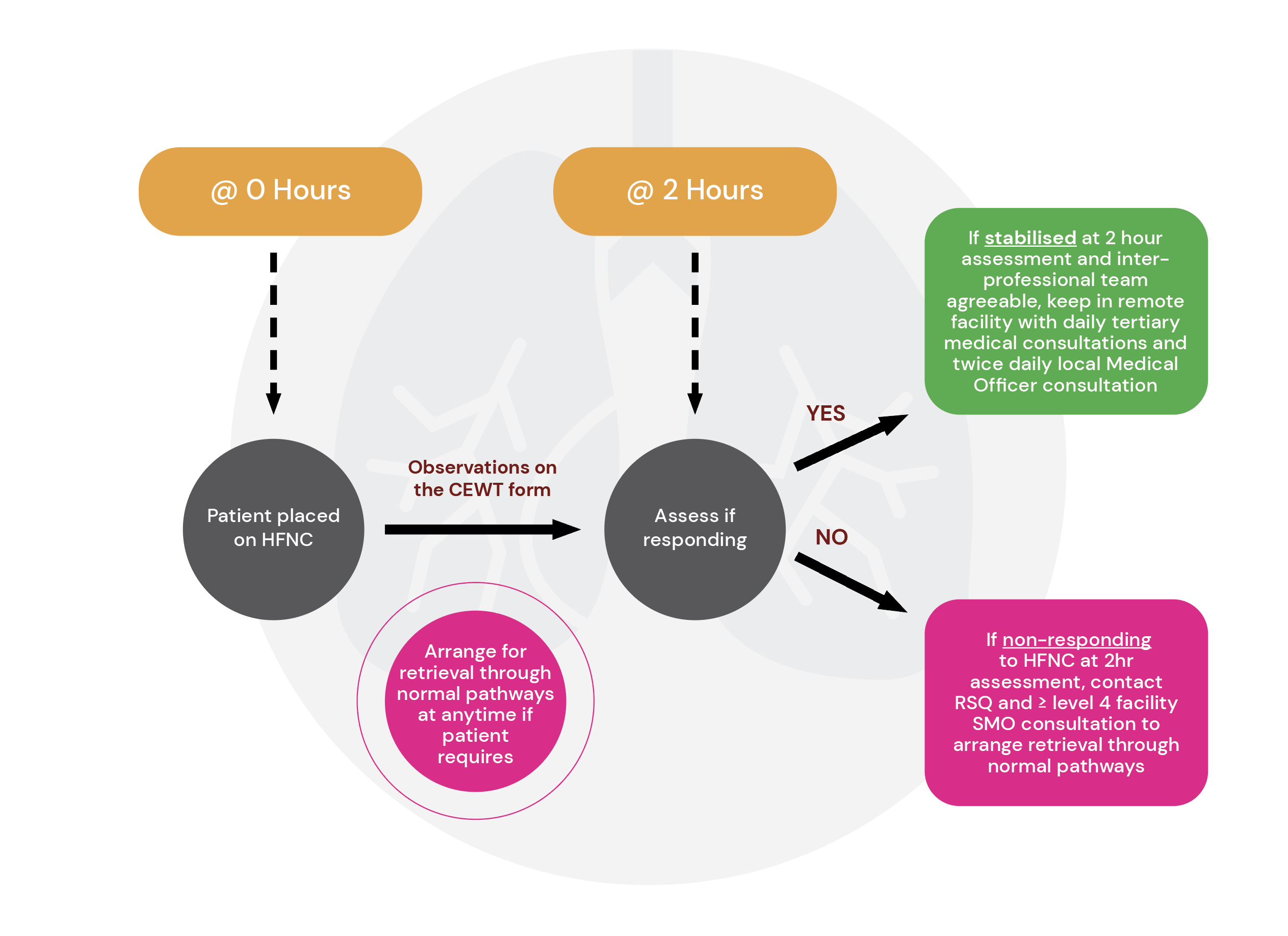
- If it is assessed at 2hrs post commencement of HFNC therapy that the patient does not require transfer to a level ≥4 CSCF facility, consultation with the level ≥4 CSCF facility is still mandated to ensure the level ≥4 CSCF facility is aware of the patient and their condition.
- If it is assessed at 2hrs post commencement of HFNC therapy that the patient has not improved or there is further deterioration in their condition, SMO consultation including both level ≥4 CSCF facility and RSQ to arrange retrieval through normal pathways.
Initiation of HFNC therapy and Equipment
Remote HFNC patient flow and Initiation
Patients who remain in Remote Facility on HFNC
Patients who remain in a remote HHS facility on HFNC therapy will have the following ongoing consultations as a minimum:
- Daily consultation with the level ≥4 CSCF team until discharged from the remote HHS facility
- Twice daily consultation by the local remote HHS treating team (including SMO,) until discharge.
Other considerations to include for a child on HFNC in a remote HHS facility include:
- Local nursing clinical leadership (Director of Nursing/ Nurse Unit Manager/ Clinical Nurse Coordinator/ Shift Team Leader) should be notified of the patient (as per normal patient status communication processes,) as soon as is practical.
- Ideally consultation between the level ≥4 CSCF facility to remote HHS facility will involve an inter-professional approach with nursing and patient/family input where possible/appropriate.
- Consultation will be conducted via the telephone at the clinician’s discretion to use videoconferencing when resources are accessible and appropriate.
- Communication throughout the tertiary consultations will use the ISBAR technique that is standardised within Queensland Health. This will be used in conjunction with the relevant prompt/advice/transfer checklist use locally in your hospital. Document all advice provided on patient management in your patient medical record. Additional local documentation tools may be used such as the CHHHS Advice/Retrieval record form. MR262 Advice/Retrieval Record Paediatrics (health.qld.gov.au)
- For all children with an acute illness, a full set of observed physiological parameters is essential and will be expected by the level ≥4 CSCF facility consulting SMO. At a minimum this includes:
- Weight
- Blood glucose level
- Respiratory rate
- Degree of respiratory distress/ work of breathing
- Oxygen saturations
- Prescribed oxygen and mode
- Temperature
- Heart rate
- Blood pressure
- Capillary refill time
- Level of consciousness/ AVPU
- Child Early Warning Tool (CEWT) score
All documentation to occur in line with local practice. This includes using the advice/prompts/clinical handover forms previously outlined and keeping a copy in the patients records in addition to providing to the higher level facility for their record keeping.
Preparation and Order
Initiation of HFNC therapy must be ordered by the treating medical officer on the AirvoOrder and Machine Observations Form MR88atb. Informed patient/carer consent must be obtained and documented. A plan for ongoing review with a paediatrician or paediatric ICU consultant must be made, as outlined above.
The facility nursing team leader is to be consulted, so that they may facilitate the care of the patient by HFNC therapy competent nursing staff, in an appropriately resourced area.
Nasogastric tubes and feeding
Infants ≤12 months – require a nasogastric tube placement with the initiation of HFNC therapy, for gastrointestinal (GIT) decompression. The NGT is to remain in situ for the duration of the therapy.
Children >12 months – may require NGT if GIT distention is an issue while on HFNC therapy and/or alternate hydration measures are required. Decision is at the discretion of the medical officer.
Equipment and setup
- HFNC therapy must be delivered by the Airvo™2 OR the AirvoTM3 device, using the appropriate AirSpiral™ circuit and Optiflow™ nasal cannula (Fisher and Paykel Healthcare Systems).
- Both Airvo™2 & 3 devices can deliver flows from 2-60L/min
- The Airvo™2 has a Junior and Adult (default) mode. The Junior mode reaches 25 L/min maximum flows and is best used on ≤12 mths of age patients. The Adult (default) mode is best used on children >12mths and flows reach 60L/min maximum.
- The Airvo™3 device has one mode only and can deliver all flows to all ages and weight ranges.
- The same AirSpiral™ circuit (900PT561) is used with all sizes of nasal cannula and on both Airvo devices.
The Table 1 outlines recommended patient flow rates
- Optiflow™ Junior 2 & 2+ nasal cannula should be secured using supplied
WigglewiNG™ ensuring a good fit into the nares but not completely obstructing the nares. See fit instruction video:
Set-up the Airvo™2 and Airvo™3 in accordance with Fisher and Paykel Airvo2 User Manual or Fisher and Paykel Airvo3 User Manual.
Flow rates & oxygenation
Flow rate determined for the commencement of HFNC therapy must be ordered by the medical officer, on the Airvo™2 Order and Machine Observations Form MR88atb. Refer to Table 2 below for current evidence-based, weight-specific flow rate recommendations. When commencing the flow, prepare the patient and carer by explaining the sensation and considering distraction techniques. Start low and increase in small increments to allow the child to adjust to the warm, humidified flow – this can occur over a few minutes or up to 10 minutes dependent on how well the child tolerates HFNC.
Note: If attempting to achieve flow settings too high for the mode and/or cannula on an Airvo2 device only, the Airvo 2 will alarm “blockage”.
Initial FiO² should be set at 0.21 (21% = room air). If SpO² < 85%, or if SpO² remains <90% after 10 minutes of HFNC therapy, then FiO² should be increased and titrated to achieve SpO² of ≥ 90%. FiO² is adjusted to maintain SpO² ≥ 90%, avoiding long periods of hyperoxia with SpO² of 100%. FiO² should be ordered on the Airvo™2 Order and Machine Observations Form MR88atb as “FiO² to maintain SpO² ≥ 90%”.
Changes to either FiO² or flow rate must be prescribed on the Airvo™2 Order and Machine Observations Form MR88atb. The clinician administering changes is to document this on the second page of the form.
Diagrams referenced above
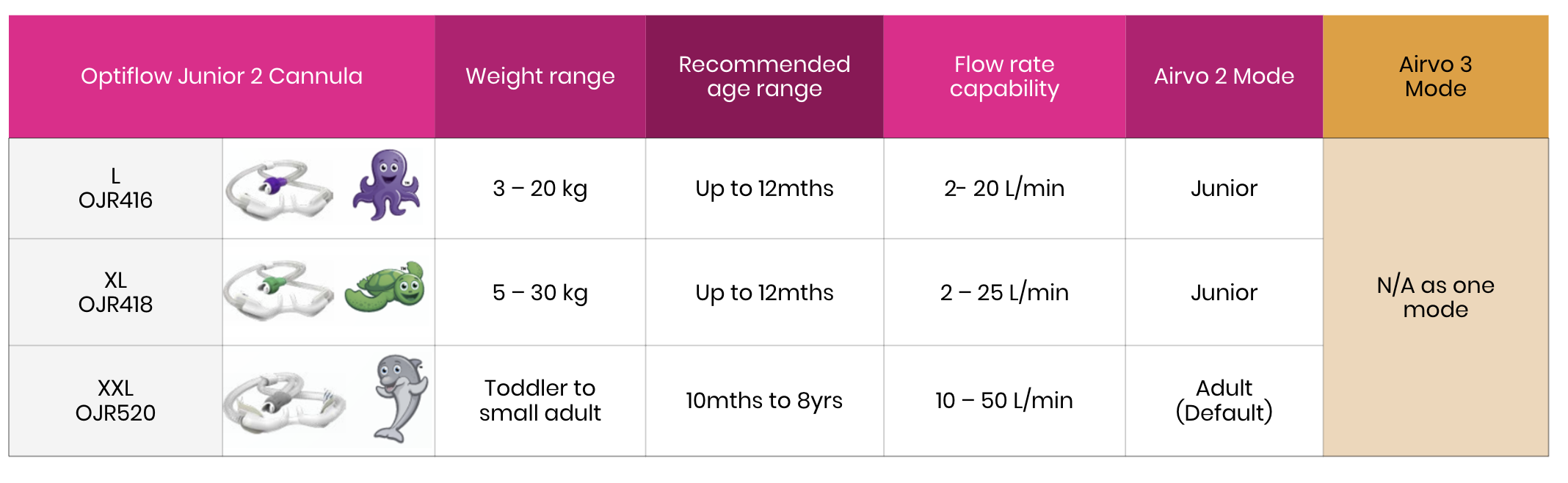
Table 1 Optiflow nasal cannula sizing guide
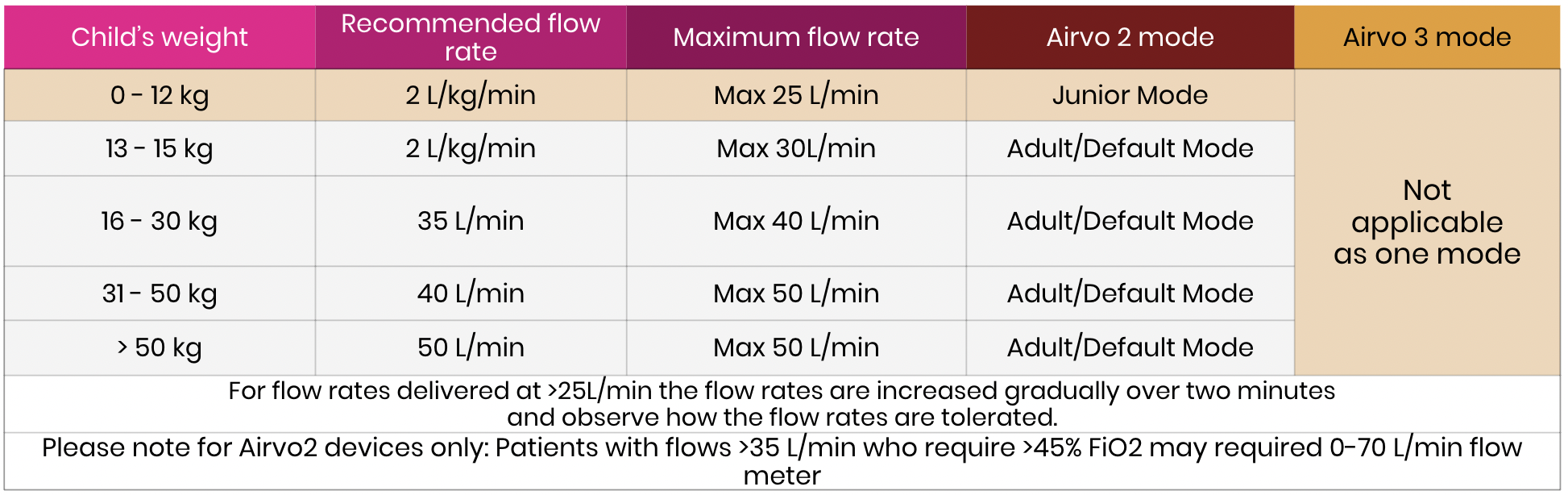
Table 2 Delivered flow rates by weight for HFNC
Diagram of the remote NHF patient flow
Management
Environment
The use of HFNC therapy means the patient is unwell and requires more and not less nursing care and clinical monitoring. The child should be cared for in a close observation area with a competently trained clinician available at all times. The environment of care may vary according to facility, time of day, staffing and skill-mix. The patient should be cared for in the location most suitable for achieving both a quiet, child friendly environment as well as adequate monitoring and access to equipment and clinicians in terms of potential deterioration; this could be in the emergency department (ED) or ward.
Following commencement of HFNC therapy in the ED, children should not be transferred to a ward setting until clinically stable. A patient is deemed ‘clinically stable’ when they meet the indicators described below in “meet the clinical indicators outlined in clinical stabilisation’. Consultation with the relevant nursing clinical leadership (for example, Nurse Unit Manager, Clinical Nurse Consultant and/or shift Team Leader) and the treating medical team should also occur before transfer to ward.
Staff Requirements
Children on HFNC outside of PICU, require a minimum of two (2) paediatric HFNC competent clinicians to be present on any given shift. (HFNC therapy competency is defined in Staff Education Below.) This may be a combination of Registered Nurse’s (RN) or RN and Enrolled Nurse (EN). At a minimum, one of these staff must be a Registered Nurse (RN). If staffing is reduced, follow local practices to ensure patient safety.
When a patient is commenced on HFNC therapy, a SMO is required to remain within the facility, until the initial 2hr trial of therapy has been completed. After this time, if the team has established that the patient has stabilised, the on-call SMO is required to arrive at the patient’s bedside within the local facilities specified guidelines regarding on-call times.
Monitoring and documentation of observations
Respiration rate, respiratory distress, oxygen (% delivered, ‘HF’ mode, actual FiO² and L/min on device screen), SpO², heart rate and conscious level must be documented at least 15 minutely for one (1) hr on commencement of HFNC therapy. Thereafter, observations are to be documented at least hourly. Continuous SpO² monitoring must stay in place. Undertake and document patient observations in accordance with the age appropriate CEWT. Undertake Paediatric Respiratory Observation Chart MR60A.7 with every set of observations.
Airvo™2 Machine observations must be documented on the Airvo™2 Order and Machine Observations Form MR88atb, and are to be undertaken hourly, at shift change, and when therapy order is changed. These include:
- Total air flow setting (L/min)
- Temperature setting (°C)
- Oxygen percentage delivered (FiO²)
- Patient skin and Optiflow™ cannula check (for pressure areas and to ensure that a slight leak is present, as complete obstruction of the nares will inadvertently create high pressure and may lead to barotrauma. Also check for dislodgement of nasal cannula, as this may result in reduced respiratory support.)
- Machine plugged in, turned on, condensation cleared
- Humidifier water chamber and sterile water bag levels (document in ‘Other’ column)
Clinical stabilisation and nursing care
Clinical stabilisation
Clinical stabilisation is defined as:
- The FiO² required to maintain SpO² in the target range (SpO² ≥90%) is ≤ 40%.
- Heart rate reduced by 15 beats per minute (bpm) or to within normal range for that infant/child’s age group.
- Respiratory rate reduced by 5-6 resps/min or to within normal range for that infant/child’s age group.
- Signs of respiratory distress/effort have improved.
Children who are unable to be stabilised with FiO² ≤ 40% should be discussed and reviewed by the level ≥4 CSCF facility and considered for transfer to the level ≥4 CSCF facility.
Nursing care
- If the medical team deem an x-ray is indicated, it is to be completed as soon as possible. Aim for within the first two hours of HFNC therapy. An x-ray should not delay the initiation of the HFNC therapy.
- Point of care pathology and/or formal pathology can be used to assess effectiveness of treatment if treating team deem it necessary.
Weaning of HFNC therapy | Clinical assessments
Weaning of HFNC therapy
Weaning of HFNC therapy must only be undertaken with guidance from a paediatrician. When weaning HFNC therapy, always maintain weight specific flows as per Table 1 and only reduce the FiO² until room air (FiO² =21%) has been achieved.
Weaning for children on HFNC room air only:
For children who commence and remain on room air (FiO² =21%) only, maintain HFNC therapy for a minimum of two hours whilst maintaining targeted saturations (90-98%). If patient remains stable, cease HFNC, remove nasal cannula and allow patient to breathe room air. If the patient desaturates, recommence HFNC at previous settings and titrate FiO² accordingly to maintain SpO² 90-98%.
Weaning for children on HFNC with FiO² >21%:
Weaning of HFNC with FiO² >21% can commence within four (4) hours, as instructed by the SMO, if the child’s clinical condition is improving:
- First, decrease the FiO² in 5% increments whilst maintaining saturations ≥ 90%.
- Once the FiO² reaches 21% and saturations have been stable ≥ 90% for one hour, flow can be ceased and nasal cannula removed.
- If infant/child desaturates < 90% resume flow with FiO² at 21%.
- If not maintaining saturations ≥ 90% increase FiO² until saturations are 90-98%.
- Once stabilised with saturations ≥ 90% for at least two (2) hours weaning can recommence.
- If the medical team deem an x-ray is indicated, it is to be completed as soon as possible. Aim for within the first two hours of HFNC therapy. An x-ray should not delay the initiation of the HFNC therapy.
- Point of care pathology and/or formal pathology can be used to assess effectiveness of treatment if treating team deem it necessary.
Clinical assessments
- If the medical team deem an x-ray is indicated, it is to be completed as soon as possible. Aim for within the first two hours of HFNC therapy. An x-ray should not delay the initiation of the HFNC therapy.
- Point of care pathology and/or formal pathology can be used to assess effectiveness of treatment if treating team deem it necessary.
Clinical deterioration
In keeping with the age appropriate CEWT, seek medical review if any of the following occurs:
- Respiratory rate increases
- Degree of respiratory distress worsens
- Requirement for FiO²>40%
- Hypoxaemia persists despite high gas flow
- Child shows signs of tiring (e.g. decreased respiratory rate and effort despite SpO² <90%)
Remember: Children have the ability to sustain physiological parameters in the face of significant illness before rapidly decompensating. Many traditionally measured observations which are relied upon in adult medicine may underestimate the severity of a child’s state.
In the case of clinical deterioration:
- Call for help/assistance as per local CEWT escalation process
- If bag and mask breaths are required always remove the nasal cannula first, to ensure adequate mask seal.
- Consider increasing flow according to the flow rate table in consultation with treating medical officer.
- Consider that if a high FiO² is used, oxygen saturation may be maintained in an infant despite the development of hypercarbic respiratory failure.
- Consider pneumothorax as a complication of HFNC therapy if there is a rapid deterioration of oxygen saturation and/or marked increased work of breathing. Exclude this by performing a chest x-ray.
- Consider blood gas analysis where clinically indicated.
HFNC therapy with feeding I hydration I inhalation
Once stable on HFNC therapy, the child should be assessed as to whether they can feed.
- Some infants can continue to breast/bottle feed, but many require feeding via a NGT
- Feeds given via the NGT can be either bolus or continuous
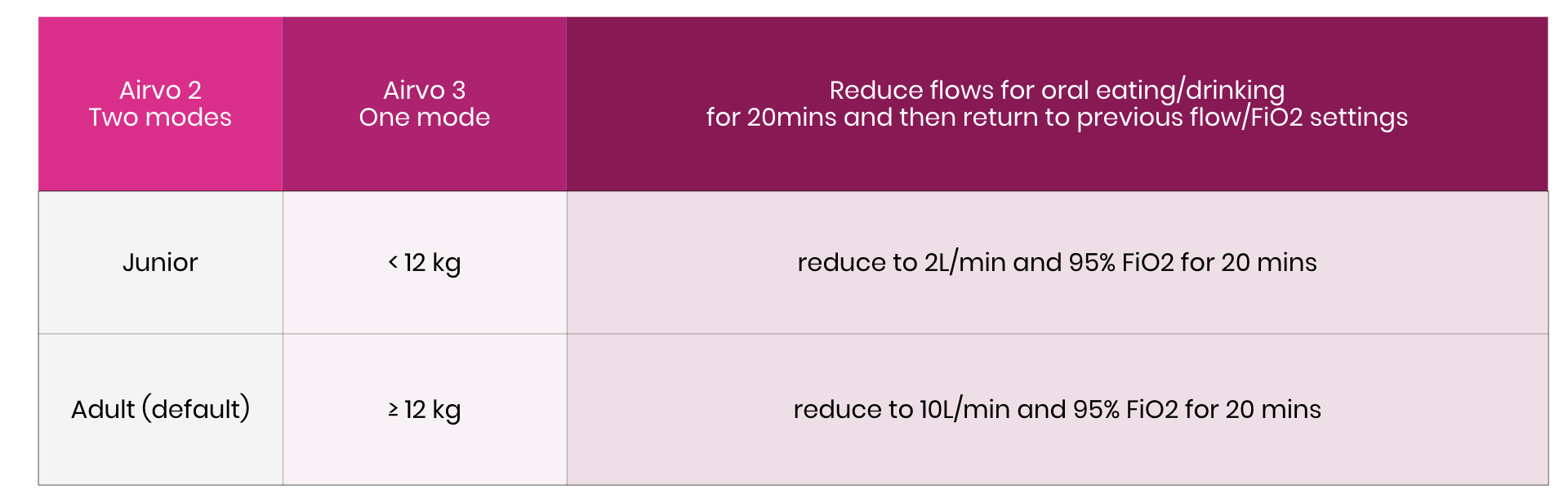
- For infants who wish to orally feed (bottle/breastfeed/drink or eat), it is preferential (particularly in ≤12 months) to reduce the HFNC therapy to low flow humidified oxygen for a short period (up to 20 minutes) as per below table
- After a maximum of 20 minutes, oral feeding should be stopped, and HFNC therapy recommenced at the previous settings.
- Older children have demonstrated that they can synchronise their swallow with eating and drinking whilst high flow is in place, with no adverse effects. However, if the child is very tachypnoeic and working very hard or has difficulty synchronising feeding/drinking with the HFNC therapy, then reduce to low flow humidified oxygen as outlined above. Reduce for a short timeframe only (up to 20 minutes) and recommence at the previous settings.
- Infants/children who do not clinically stabilise within 2 hours or who do not tolerate NGT feeds should have an I.V. inserted to receive hydration. Aim for patient to be managed with 2/3 fluids maintenance.
Inhalation therapy with HFNC
Children on HFNC, requiring inhalation therapy via a nebuliser or multidose inhaler (MDI) are to perform the following:
- MDI’s:
- Remove nasal cannula to ensure a good seal for MDI and administer inhalation medication
- Following inhalation completion replace nasal cannula and continue HFNC at previous settings.
- Nebulisers:
- Stop HFNC and remove nasal cannula for greater seal to skin and administer nebuliser OR
- keep cannula in place and reduce flows to low flow humidified settings for duration of nebuliser. These settings are in accordance to the AIRVO2 and 3 mode differences:
- Following nebuliser completion replace nasal cannula and continue HFNC at previous settings.
Note:
- When setting up HFNC therapy, ensure that the Airvo device is placed below patient head height to prevent water from entering nasal cannula.
- Manage excess condensation in tubing by disconnecting from patient and lifting the patient end of the tube to allow the condensation to run into the water chamber.
- When removing nasal cannula, then replacing (e.g., for MDI use), ensure tubing is free from water before re-applying to child
Cleaning of the Airvo 2 or Airvo 3 | Transfer on Airvo systems
Transfer of Airvo systems
Intrahospital transfers, such as movement from ED to ward/radiology can occur with the use of the Airvo™3 battery built-in system that will last up to 40 minutes. If the patient requires oxygen, ensure the change over from wall oxygen outlet to cylinder oxygen occurs using the dual high pressure oxygen setup.
Inter-hospital transfers and mode of respiratory support will be as per the decision of the retrieval team to ensure respiratory support mode will be functional for entire transport.
NB: The Airvo™2 device does not allow HFNC therapy delivery during transport unless it is connected to power or an external battery.
In the event of transfer to a higher care facility (e.g., Level 4), clinical handover must occur between two HFNC competent nurses. I.e. HFNC competent nurse at Remote HHS facility, and HFNC competent nurse at level ≥4 CSCF facility.
Cleaning of the Airvo 2 or Airvo 3
The Airvo Humidifier requires cleaning and disinfection between patients. Follow the instructions in the Fisher and Paykel Airvo2 Disinfection Kit Manual or Fisher and Paykel Airvo3 Manual – section 8. Keep the orange disinfection tubing connected post disinfection cycle, to ensure the Airvo does not collect dust inside the equipment.
Humidifier chamber, circuits and nasal cannula are single patient use. They are to be disposed of in general waste. If a patient is receiving HFNC therapy for an extended period, the consumables are to be changed every seven (7) days.
Staff Education
In order to care for a patient receiving HFNC therapy, medical officers and nursing staff must be competent in the delivery and management of HFNC therapy.
Competence may be demonstrated by:
– Attendance at in-service or completion of a short (20 min) HFNC therapy inservice, AND successful completion of Airvo 3 Competency Checklist.
This is a one-off requirement to be completed prior to using HFNC therapy. It is the individual’s responsibility to maintain competency after initial training.
Clinicians involved in the care of a patient receiving HFNC therapy must also be competent in the insertion and management of NGT for paediatric patients. Undertake NGT cares in accordance with the local practice guidelines.
Resources and References
Resources and References
Babl, F., Franklin, D., et al. Enteral Hydration in High-Flow Therapy for Infants with Bronchiolitis: Secondary Analysis of a Randomized Trial. Journal of Paediatrics and Child Health. February 2020.
CHQHHS Guideline Care of the Paediatric Patient requiring Nasal High Flow Therapy in PICU
Fedor, K. L. (2017). Noninvasive Respiratory Support in Infants and Children. Respiratory Care, 62(6), 699-717. doi:10.4187/respcare.05244
Franklin D, Babl FE, George S, et al. Effect of Early High-Flow Nasal Oxygen vs Standard Oxygen Therapy on Length of Hospital Stay in Hospitalized Children With Acute Hypoxemic Respiratory Failure: The PARIS-2 Randomized Clinical Trial. JAMA. 2023;329(3):224–234. doi:10.1001/jama.2022.21805
Franklin D, Babl F, Schlapbach L, Oakley E, Craig S, Neutze J, Furyk J, Fraser J, Jones M,Whitty J, Dalziel S, Schibler A. (2018) A Randomised Trial of High-Flow Oxygen Therapy in Infants with Bronchiolitis. The New England Journal of Medicine; 378:1121-31.
Franklin, D., Shellshear, D., et al. High Flow in Children with Respiratory Failure – a Randomised Controlled Pilot Trial – A Paediatric Acute Respiratory Intervention Study (PARIS). Journal of Paediatrics and Child Health. 2021;2: 273-281.
Hutchings FA, Hilliard TN, Davis PJ. Heated humidified high-flow nasal cannula therapy in children. Archives of Disease in Childhood 2015;100:571-575.
Long E, Babl FE, Duke T. Is there a role for humidified heated high-flow nasal cannula therapy in paediatric emergency departments? Emerg Med J 2016;33:386-389.
Mayfield, S, Boggossian, F, O’Malley,L, and Schibler, A.(2014) Nasal High Flow oxygen therapy for infants with bronchiolitis: Pilot Study: Journal of Paediatric Child Health 50: 373-378.
Mikalsen, I. B., Davis, P., & Øymar, K. (2016). High flow nasal cannula in children: a literature review. Scandinavian Journal Of Trauma, Resuscitation And Emergency Medicine, 2493. doi:10.1186/s13049-016-0278-4
O’Brien, S., Haskell, L., Schembri, R., Gill, F.J., Wilson, S., Borland, M.L., Oakley, E., Dalziel, S.R. and (2022), Prevalence of high flow nasal cannula therapy use for management of infants with bronchiolitis in Australia and New Zealand. J Paediatr Child Health, 58: 2230-2235.
Schlapbach, L. J., Schaefer, J., Brady, A., Mayfield, S., & Schibler, A. (2014). High-flow nasal cannula (HFNC) support in interhospital transport of critically ill children. Intensive Care Medicine, 40(4), 592-599. doi:10.1007/s00134-014-3226-7
Mündel T, Feng S, Tatkov S, Schneider H. Mechanisms of nasal high flow on ventilation during wakefulness and sleep. J Appl Physiol (1985). 2013 Apr;114(8):1058-65. doi: 10.1152/japplphysiol.01308.2012. Epub 2013 Feb 14. PMID: 23412897; PMCID: PMC3633436.
Parke RL, Eccleston ML, McGuinness SP. The effects of flow on airway pressure during nasal high-flow oxygen therapy. Respir Care. 2011 Aug;56(8):1151-5. doi: 10.4187/respcare.01106. Epub 2011 Apr 15. PMID: 21496369.