
Pre-school wheeze Emergency management in children in the remote context
Pre-school wheeze is also referred to as Reactive airways disease. Wheeze is a very common presentation in children that is usually caused by intercurrent viral infection or other environmental triggers.
The term asthma is not used to describe a wheezing illness in pre-schoolers as there is insufficient evidence that the pathophysiology is similar to that of asthma in older children and adults.
Key Points
- Wheezing in preschool-aged children is due to a heterogeneous group of diseases.
- A thorough assessment and continuous review is necessary for each child during their presentation.
- Steroids are not indicated in pre-school children who present for the first time or infrequently with a mild to moderate wheeze.
- Wheezing illnesses can be life-threatening.
Background
Wheeze is a continuous high-pitched sound with musical quality emitting from the chest during expiration, with increased work of breathing
Pre-school wheeze is also referred to as reactive airways disease
Pre-schoolers commonly experience wheeze during discrete time periods, often in association with clinical evidence of a viral infection (such as rhinovirus, RSV, coronavirus, human metapneumovirus, parainfluenza virus and adenovirus) with symptoms absent between episodes
Repeated episodes tend to occur seasonally, and it usually declines over time disappearing by six years of age. This is known as an episodic viral wheeze
Viral infection is a common trigger but other triggers include tobacco smoke, allergen exposure, mist, crying, laughter and exercise.
Risk factors for a future diagnosis of asthma include:
- onset of wheeze over the age of 18 months
- personal history of atopy e.g. eczema
- maternal asthma
Assessment, History & Examination
Assessment
The purpose of assessment (history taking and physical examination) is to:
- confirm a wheezing disorder
- identify symptom pattern, severity and possible trigger factors
- look for features suggestive of an alternative diagnosis or associated condition
History
History should include specific information on:
- the wheeze, other noises and features of respiratory distress
- family history (including mother and sibling/s) of asthma and atopy
- smoking status of household members
All health professionals have a role in advocating for their patients by advising parents about the increased risk of wheezing associated with parental smoking.
Examination
- Assess child as per recommended triage category
- General appearance, mental state and level of respiratory distress are best markers of illness severity.
- Signs of respiratory distress in pre-school children include accessory muscle use, abdominal breathing, intercostal recession, subcoastal recession and tracheal tug.
- Poor gas exchange and decreased saturations may be a result of severe airway obstruction due to bronchoconstriction, airway oedema and/or mucous plugging.
 |
ALERT – Wheeze may be absent due to severe airway obstruction or extreme fatigue. A “silent chest” (chest with little or no breath sounds) is a warning sign of life-threatening respiratory failure and/or respiratory arrest. |
 Click the table to enlarge
Click the table to enlarge
 Click the table to enlarge
Click the table to enlarge
Differential Diagnosis
Wheeze is due to the narrowing of intrathoracic airways and expiratory flow, irrespective of the underlying mechanism.
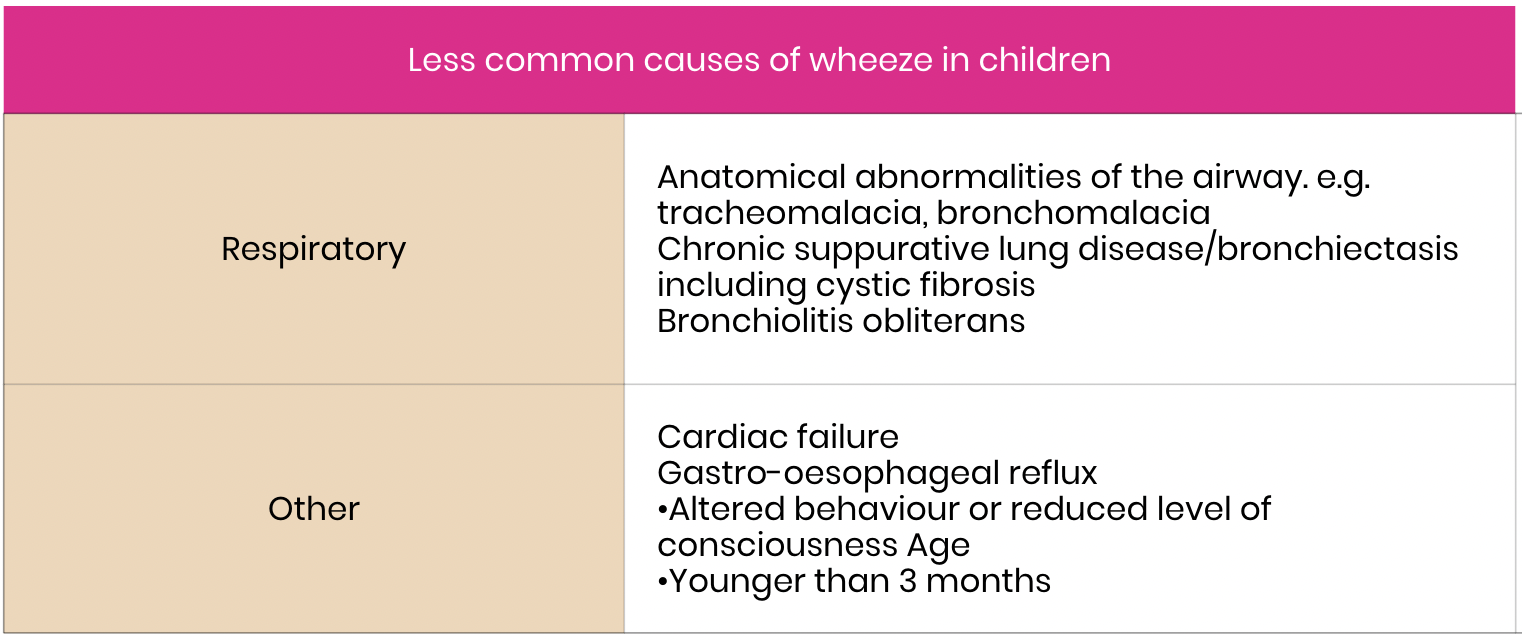
Less commonly, there are alternative reasons for a child to wheeze. Consider further investigation if the assessment (history and examination) identifies any unusual features that may allude to the differential diagnoses outlined in the following table.
 click on table to enlarge
click on table to enlarge
Investigations
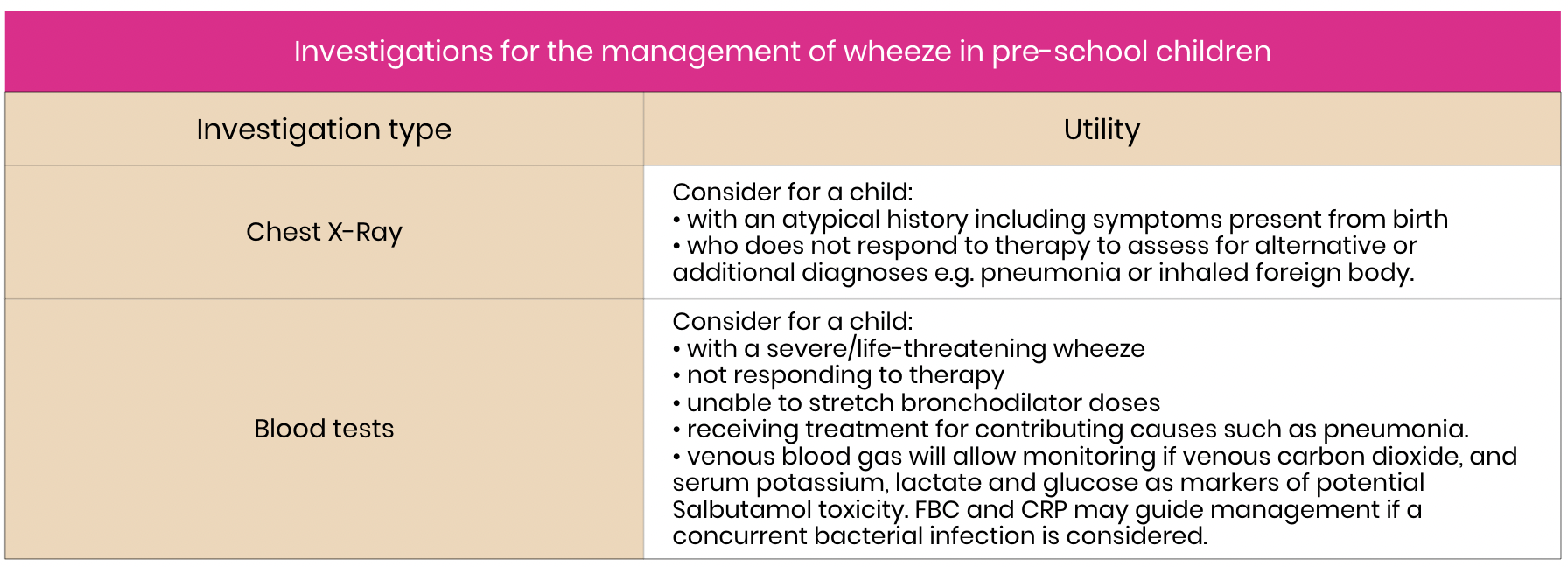
Investigations are not routinely recommended, including viral PCR testing – will not alter management.
 Click table to enlarge
Click table to enlarge
Acute Management including Bronchodilators
Acute Management
Refer to the Flowchart below for a summary of the recommended emergency management and medications for a pre-school child with a wheezing illness.
Management comprises medications targeted at
- relieving acute bronchospasm
- alleviating lower airway inflammation
- providing respiratory support in the form of oxygen and non-invasive ventilation.
Steroids are not indicated in preschool children who present for the first time or infrequently with a mild to moderate wheeze.
Repeated clinical assessment following each treatment is essential to determine the change in clinical symptoms (improvement/no change/deterioration). This should be well documented in the patient clinical notes.
Bronchodilators
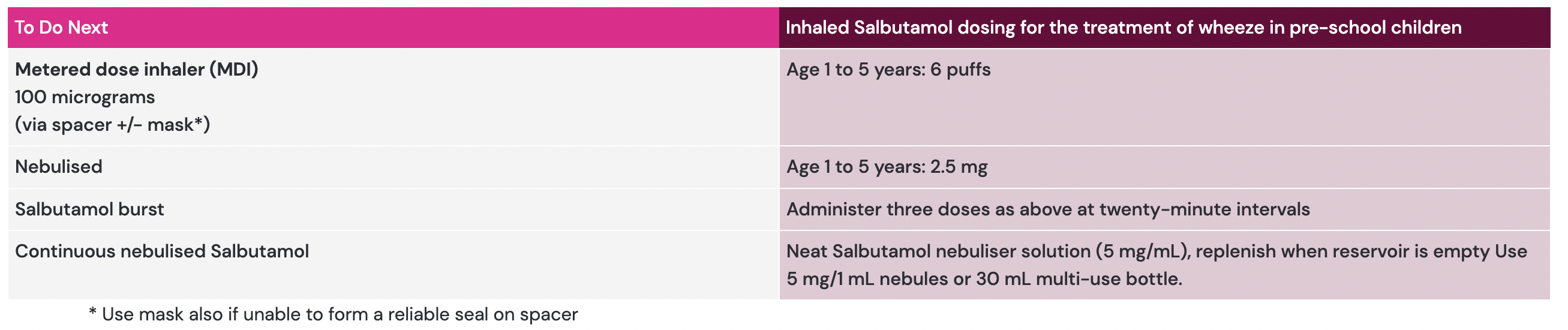
Salbutamol (short acting inhaled beta2 agonist) is recommended for all pre-schoolers with wheeze.
Monitor oxygen saturations continuously if administering Salbutamol more often than every two hours. Bronchodilators may produce a paradoxical effect in children with underlying structural abnormalities such as bronchomalacia or tracheomalacia.
 click on table to enlarge
click on table to enlarge
|
ALERT- Consider cardiac disease. In infants with the following: Cumulative Salbutamol doses can cause agitation, tremor, tachycardia, tachypnoea and rarely, hypertension. Raised lactate, hypokalaemia and raised glucose on VBG are markers of Salbutamol toxicity. |
Weaning Salbutamol
Stretching the time between Salbutamol doses should be based on an assessment on the child. This should be done in collaboration with the child and caregiver and include:
- respiratory distress: decreased work of breathing (subcostal & intercostal recession/ tracheal tug /nasal flaring)
- activity level: decreasing lethargy, increasing alertness
- respiratory rate: decreasing to within normal limits for age
- heart rate: decreasing to within normal limits for age
- speech: able to talk in sentences
- auscultation: air entry improved, wheeze reduced or appearance of wheeze in previously quiet chest (note wheeze alone is not an indication for Salbutamol)
- cough: reduction or change in cough i.e. becomes looser
- oxygen saturations: increasing oxygen saturations and decreasing oxygen requirement
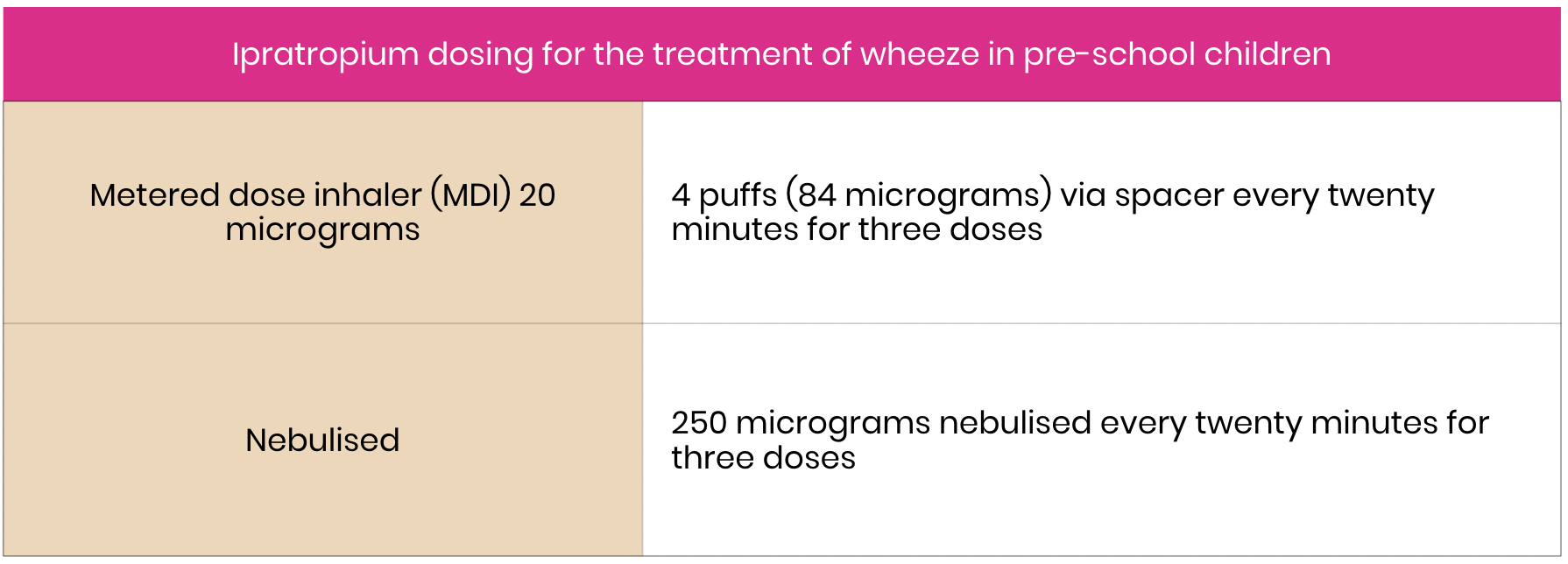
Ipratropium bromide
- Not routinely recommended as there is insufficient evidence to support use.
- Consider for children with severe symptoms following Salbutamol MDI or in combination with Salbutamol in nebuliser reservoir.
Click on the image to enlarge
MDI/Nebuliser
MDI and spacer vs nebuliser
MDI usually preferred as:
- faster (nebuliser requires a child to sit still for at least 10 minutes).
- less facial and oropharyngeal deposition of medication (nebuliser delivers at best 10% of the prescribed + drug to the lungs and child may experience side effects of systemic absorption such as tachycardia and tremor)
Nebuliser is recommended for children who are struggling with their breathing and/or not able to co-ordinate taking a deep breath through the spacer.
How to use a spacer
- Prime spacer before use to negate electrostatic charge (and optimise drug delivery) with 10 Salbutamol puffs.
- Shake MDI before each puff. Administer one puff at a time into the spacer (+/- face mask).
- The child clears the medication from the spacer by taking four breaths following each puff.
Steroids
Steroids are recommended for pre-school children with wheeze with:
- frequent episodes
- ongoing bronchodilator use more frequently than every two hours
- severe or life-threatening symptoms
- a requirement for intensive care unit admission
 click on image to enlarge
click on image to enlarge
Consider steroids for pre-school children with a history suggestive of an asthma phenotype e.g. atopy and maternal family history of asthma.
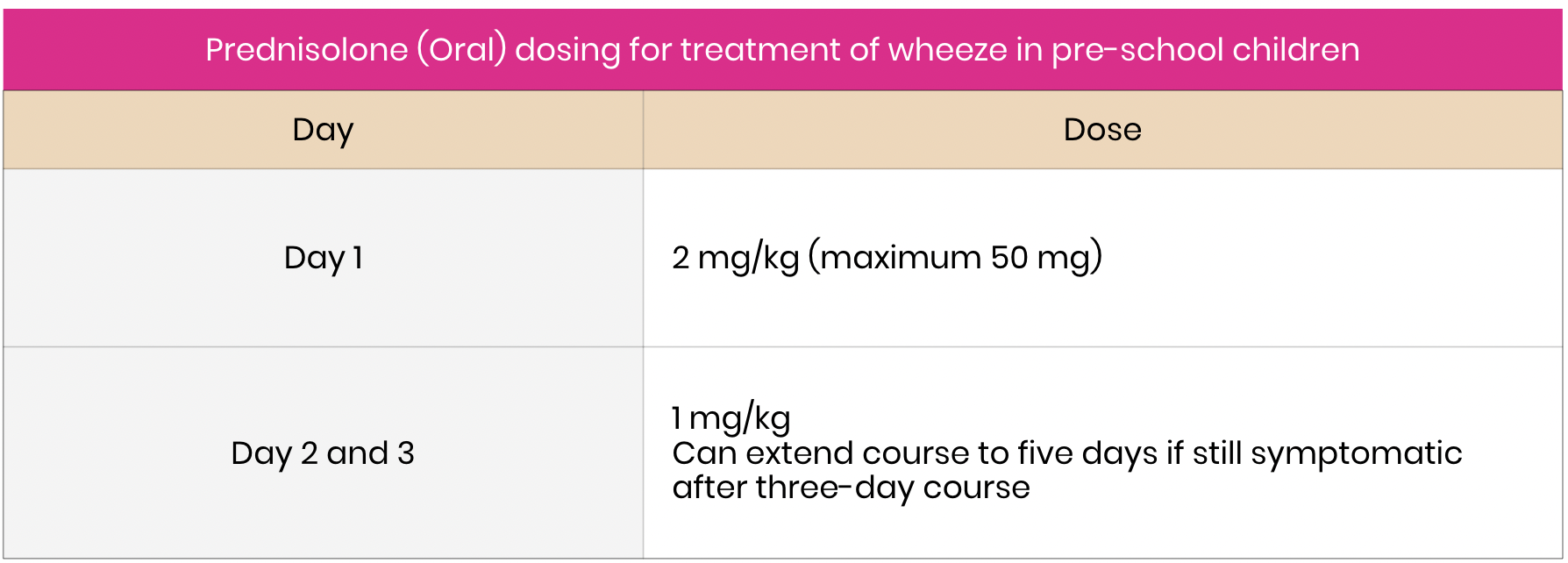
The systemic steroid of choice is oral Prednisone/Prednisolone.
Studies have shown that Dexamethasone may be a suitable alternative steroid. In a recent paediatric study, a single 0.3 mg/kg dose of Dexamethasone was found to be as effective as a three-day course of Prednisone to Prednisone 0.1 mg/kg for three days.15 However, Dexamethasone suspension is not readily available in the community or non-tertiary hospitals.
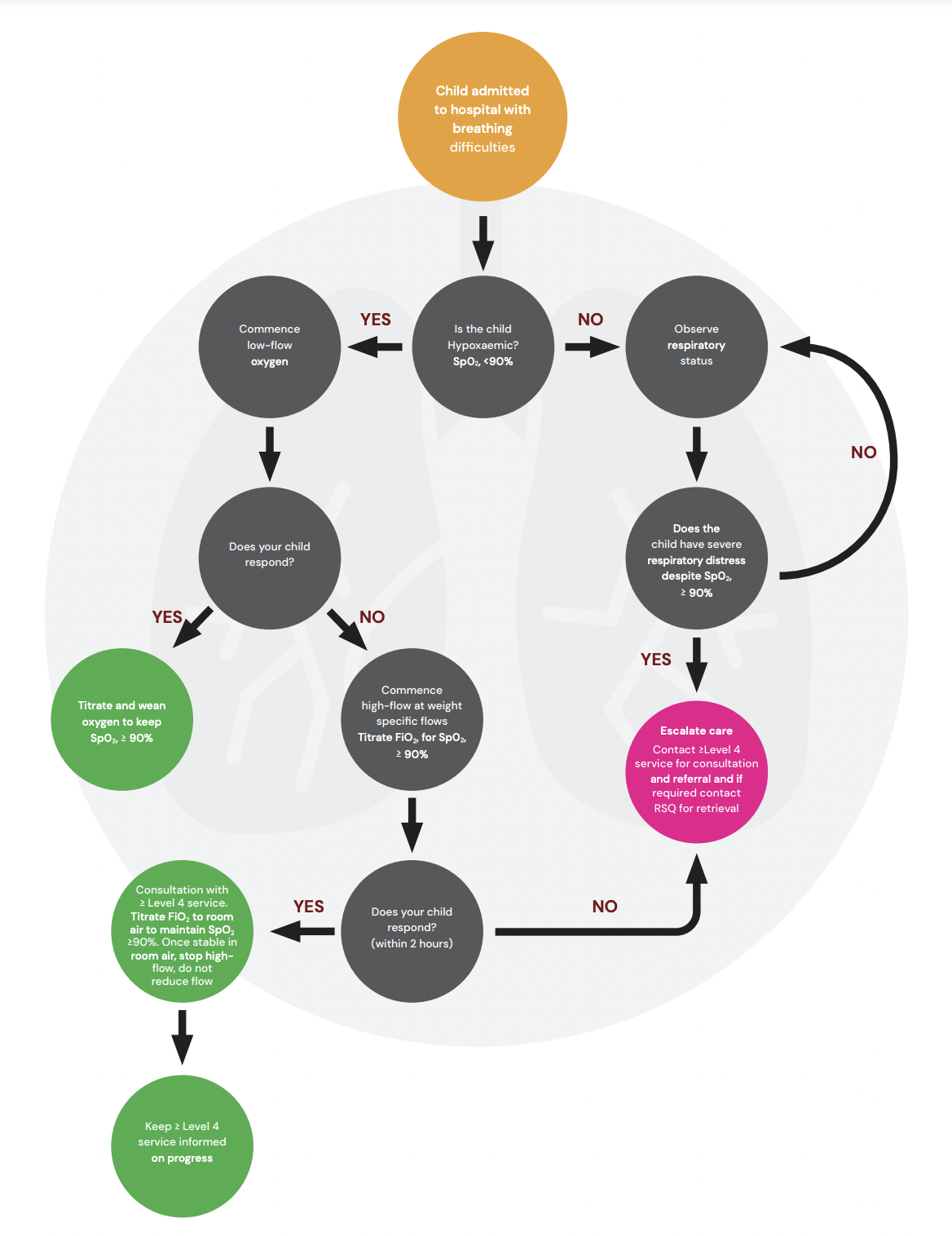
Oxygen (including HFNC therapy)
Target oxygen saturations (SpO2) and the use of low and high-flow oxygen therapy are highly variable depending upon local practice and resource availability. Follow local policies where available. Continuous oximetry should be performed in children requiring oxygen.
 click on image to enlarge
click on image to enlarge
Oxygen Therapy Flow Chart
 click on digram to enlarge
click on digram to enlarge
HFNC therapy and ongoing bronchodilator therapy
Providing bronchodilator therapy at the same time as HFNC therapy is challenging. A specific circuit (preferred) or a transient decrease to low flow oxygen is required. Where a circuit is not available and the child is too unwell to remove HFNC therapy, a bolus or infusion of salbutamol IV is recommended.
Intravenous medications
Intravenous medications
Magnesium sulphate
 |
ALERT – Seek senior emergency/paediatric input as per local practice for child requiring magnesium sulphate. Consider contacting RSQ for paediatric critical care advice. |
Consider in child with severe/life-threatening respiratory distress who is not responding to inhaled bronchodilators.
Magnesium sulphate is thought to act by decreasing the uptake of calcium by bronchial smooth muscle cells, which leads to bronchodilation. In addition, it may have a role in inhibiting mast cell degranulation, which reduces inflammatory mediators.18,19 There is no clear evidence to support use for the treatment of preschool wheeze.11
Consider in child with severe/life-threatening respiratory distress who is not responding to inhaled bronchodilators.
Magnesium sulphate is thought to act by decreasing the uptake of calcium by bronchial smooth muscle cells, which leads to bronchodilation. In addition, it may have a role in inhibiting mast cell degranulation, which reduces inflammatory mediators. There is no clear evidence to support use for the treatment of preschool wheeze.
|
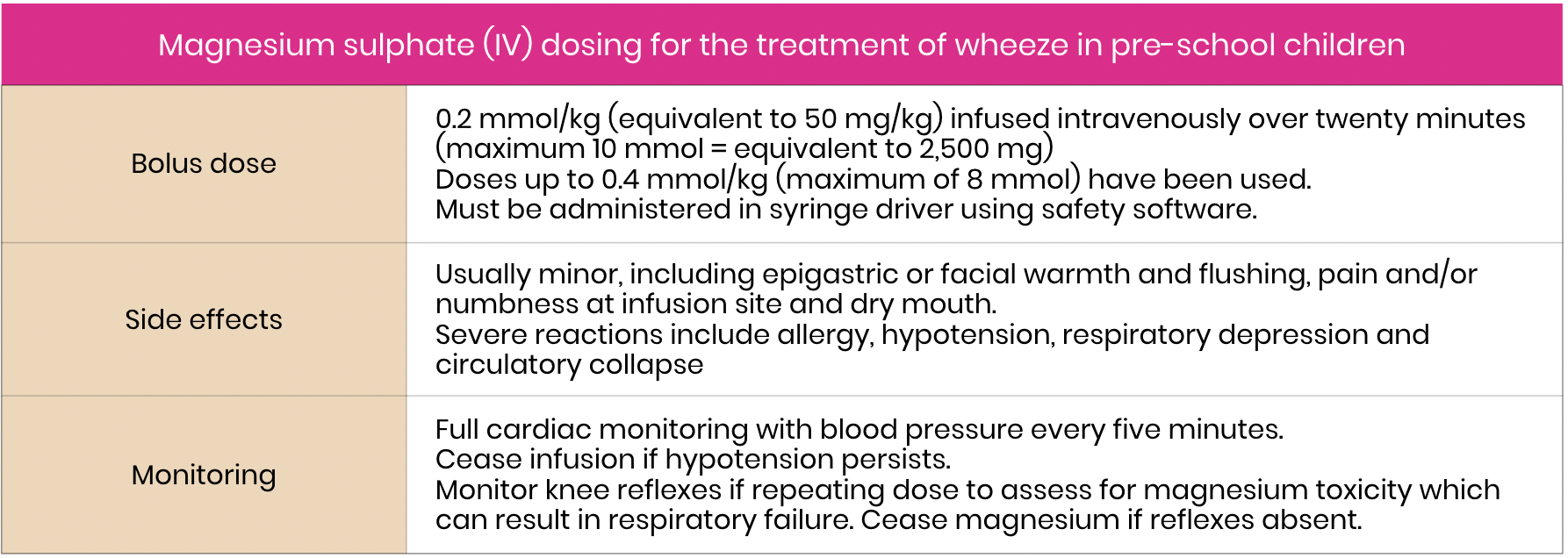
ALERT – Prescribe Magnesium in mmols and administer using safety software syringe drivers. |
Administer Magnesium sulphate using safety software syringe drivers with a standard concentration of 0.5 mmol/ml. e.g. a 10 kg child, the Magnesium sulphate dose is 0.2mmol/kg = 2 mmol.
This translates to 4ml of 0.5 mmol/ml solution and must be administered through a safety software syringe driver over 10 – 20 minutes to minimise the risk of too rapid administration and dosing errors.
 click table to enlarge
click table to enlarge
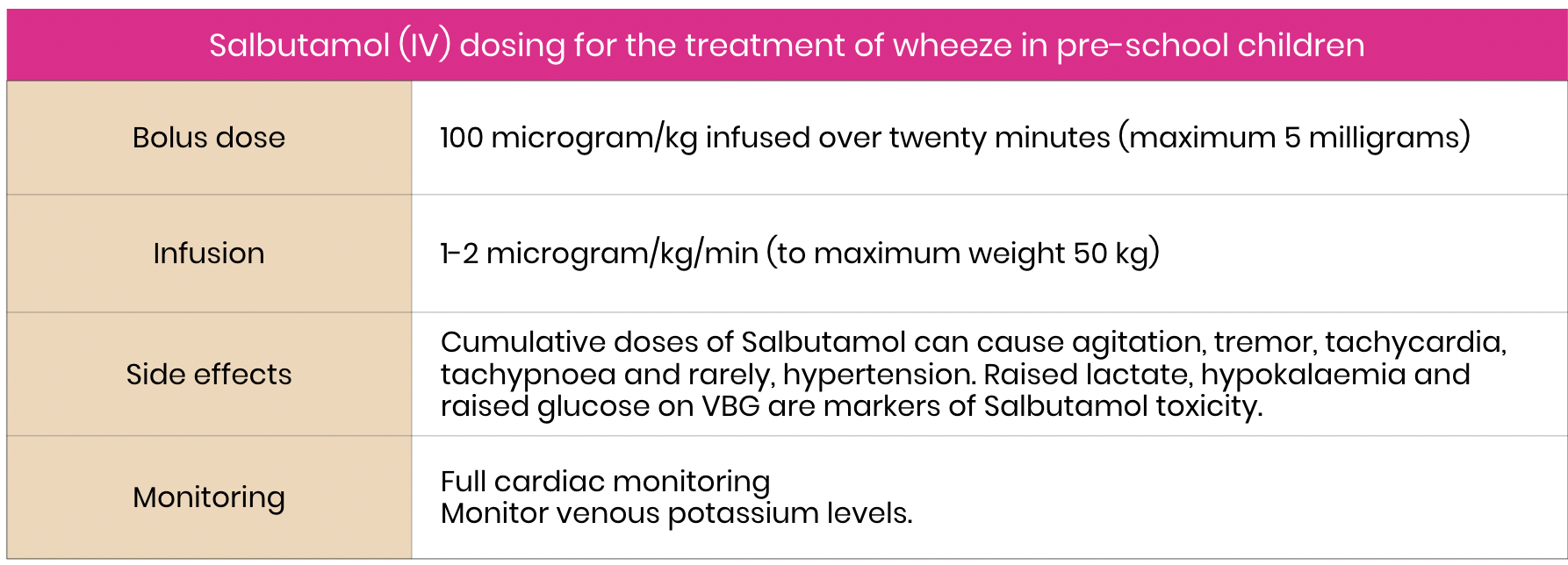
Intravenous salbutamol
|
ALERT – Contact paediatric critical care specialists (via RSQ) for children requiring Salbutamol IV. |
Salbutamol IV is only recommended for children with a very severe acute wheeze.
Administer an initial bolus dose and monitor closely for signs of Salbutamol toxicity. Slow or cease infusion is significant concerns. Evaluate the clinical response to this initial dose and consider progression to a Salbutamol IV infusion.
 click table to enlarge
click table to enlarge
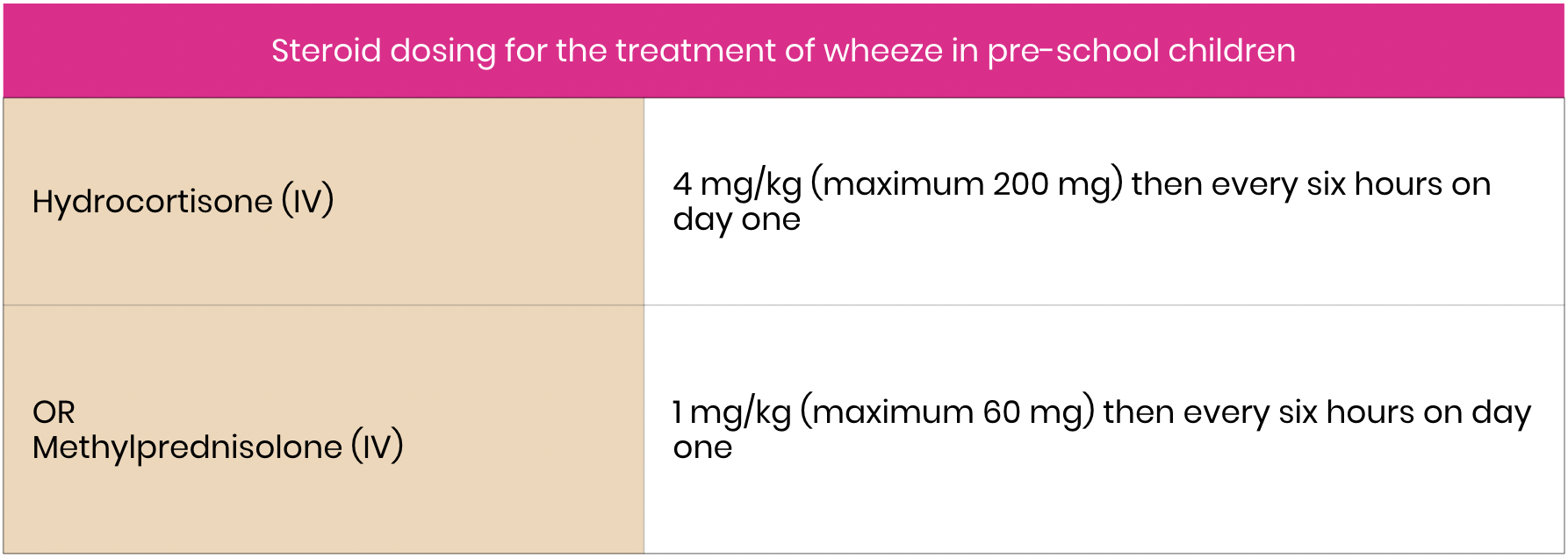
Intravenous steroids
|
ALERT – Seek senior emergency/paediatric input as per local practice for children requiring steroids IV. Consider seeking paediatric critical care input (onsite or via RSQ). |
Consider in a child with severe wheeze who cannot tolerate oral medication or has a decreased conscious level.
 click on table to enlarge
click on table to enlarge
Medications not routinely recommended
The following medications are not routinely recommended in the acute management of pre-school wheeze:
- hypertonic saline
- oral beta2 agonists (e.g. Salbutamol syrup) due to systemic side effects
- inhaled corticosteroids
- intermittent montelukast

Escalation and Advice for Remote Hospitals
For greater detail refer to:
- Remote Management of high flow nasal cannula in paediatric patients
- Escalation/Consultation to HFNC for deteriorating patient
Consultation with external paediatric team when:
- Child has specific risk factors (detailed earlier)
- Escalation to HFNC required
- severe and not responding to treatment
- requiring Salbutamol IV
- if considering NIV or intubation
Physiological triggers including the following as a guide:
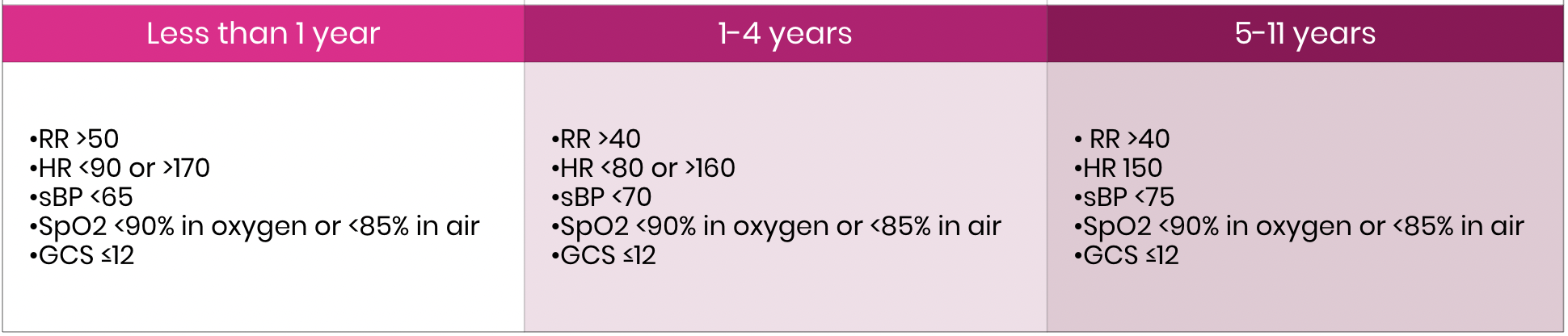
click on table to enlarge
 |
Please ensure the local remote hospitals Senior Medical Officer (or similar) is aware/involved. |
Escalation/Consultation to HFNC therapy for deteriorating patient
HFNC therapy may help avoid intubation but can also provide pre-oxygenation whilst preparation for inevitable intubation is underway.
A randomised controlled study showed that HFNC therapy does not reduce the hospital length of stay but is safe to be used in pre-school wheeze. The outcome of this study suggests that standard oxygen should be the first line oxygen therapy and HFNC only be used if escalation of care is required using the following criteria.
Escalation: Escalation of respiratory support from standard oxygen to HFNC therapy should be considered if one or more of the following is present:
- heart rate remains >160min for longer than 2 hours
- respiratory rate remains >45/min for longer than 2 hours
- oxygen requirement on SOT exceeds standard oxygen therapy (2 L/min by nasal prong, or 8L/min by facemask) to maintain SpO2 ≥90%
- increased work of breathing requiring escalation of respiratory support and assessed as moderate to severe respiratory failure
Consider transfer to higher level of care if on HFNC and if one or more of the following is present:
1. Heart rate remains >160/min for longer than 2 hours start HFNC
2. Respiratory rate remains >45/min for longer than 2 hours since start of HFNC therapy
3. oxygen requirement on HFNC exceeds FiO2 > 40% (dependant on hospital standard policy) to maintain SpO2 ≥90%
4. The hospital internal Early Warning Tool (CEWT) calls for medical review
For all paediatric critical care advice and assistance contact any of the following:
- Level ≥4 CSCF facility consultation MUST be sought within 2 hours of HFNC therapy treatment commencing.
- The level ≥4 CSCF facility to your HHS facility consultation should occur at the Senior Medical Officer (SMO) level from both facilities.
- Referring clinician to contact their relevant level ≥4 CSCF facility for consultation – this should be Senior Medical Officer (SMO) level referral at both facilities.
- If a retrieval is clearly required in the first instance contact RSQ (1 300 799 127) to link all relevant parties together including:
- referring SMO from remote hospital
- local level ≥4 CSCF facility
- relevant local Intensive Care Specialist – dependent on the patient’s condition
- A patient must be accepted at an SMO level at the receiving facility.
- If it is assessed at 2hrs post commencement of HFNC therapy that the patient does not require transfer to a level ≥4 CSCF facility, consultation with the level ≥4 CSCF facility is still mandated to ensure the level ≥4 CSCF facility is aware of the patient and their condition.
- If it is assessed at 2hrs post commencement of HFNC therapy that the patient has not improved or there is further deterioration in their condition, SMO consultation including both level ≥4 CSCF facility and RSQ to arrange retrieval through normal pathways.
These services will provide:
- consultation and access to general paediatric +/- paediatric critical care telephone advice
- coordinate the retrieval of a critically unwell child.
Disposition
Consider discharge from ED when ALL of the following are met:
- well, active child requiring Salbutamol no more frequently than every three hours
- Sp02 greater than or equal to 94%
- normal hydration and toleration of diet and fluids
- parent/caregiver can safely manage the child at home, return in event of deterioration and access further medication.
Consider a longer period of observation despite meeting the clinical discharge criteria for the children with a previous critical care admission or previous sudden deterioration.
Follow-up with GP or Paediatrician within a week, depending upon the course of the illness. (See discharge fact sheets below).
Consider admission when the following occurs:
- ongoing respiratory distress with failure to respond to initial treatment or requiring oxygen
- clinical deterioration with a need to escalate treatment
- unable to stretch bronchodilators within four hours of ED presentation OR below
- failure to progress and wean bronchodilators to every three hours in 12 – 24 hours (consider poor bronchodilator response, suboptimal administration or alternative diagnosis)
- persisting supplemental oxygen requirement
- previous critical care admission or previous sudden deterioration
- unable to get to a hospital within 30 minutes
- social factors impacting upon ability to monitor and supervise child at home
On discharge, parent/caregiver should be provided with a Pre-school Wheeze Factsheet and advised to seek medical help prior to next appointment if worsening symptoms.
Follow-up with GP within two to three days or earlier if symptoms worsen.
When to consider discharge from ward
An assessment of the family’s ability to safely manage the child at home with pre-school wheeze prior to discharge.
On discharge a child should be provided with:
- Discharge letter
- Pre-school Wheeze Disease Education Checklist (PDF)
- Wheeze Action Plan
- Pre-school Wheeze factsheet
- Puffers and Spacers factsheet
Diagrams and important tables referenced
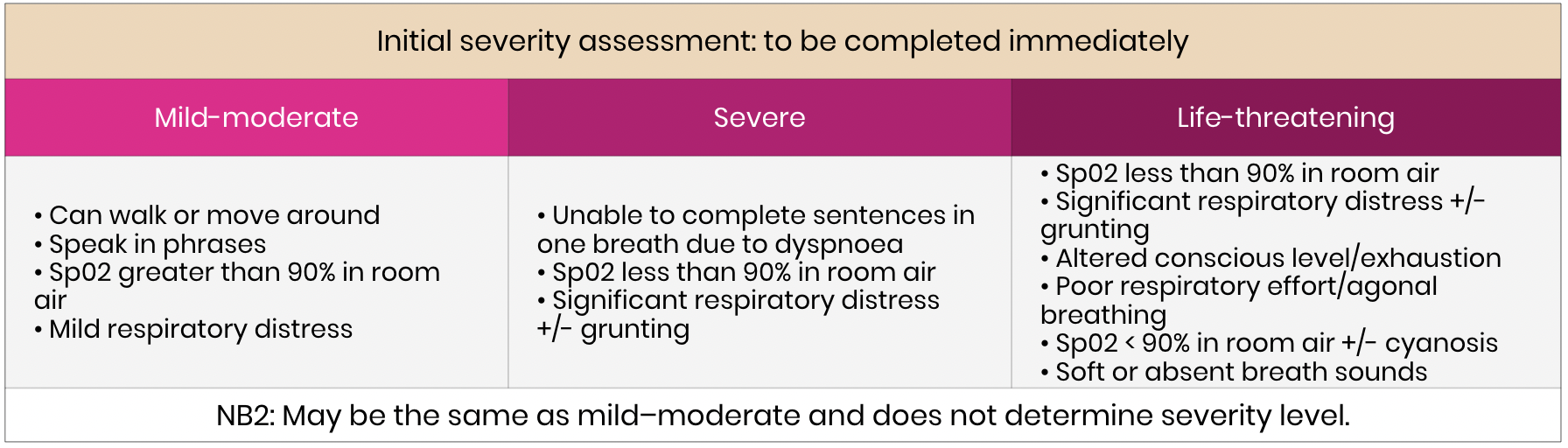
 Initial severity assessment: to be completed immediately
Initial severity assessment: to be completed immediately
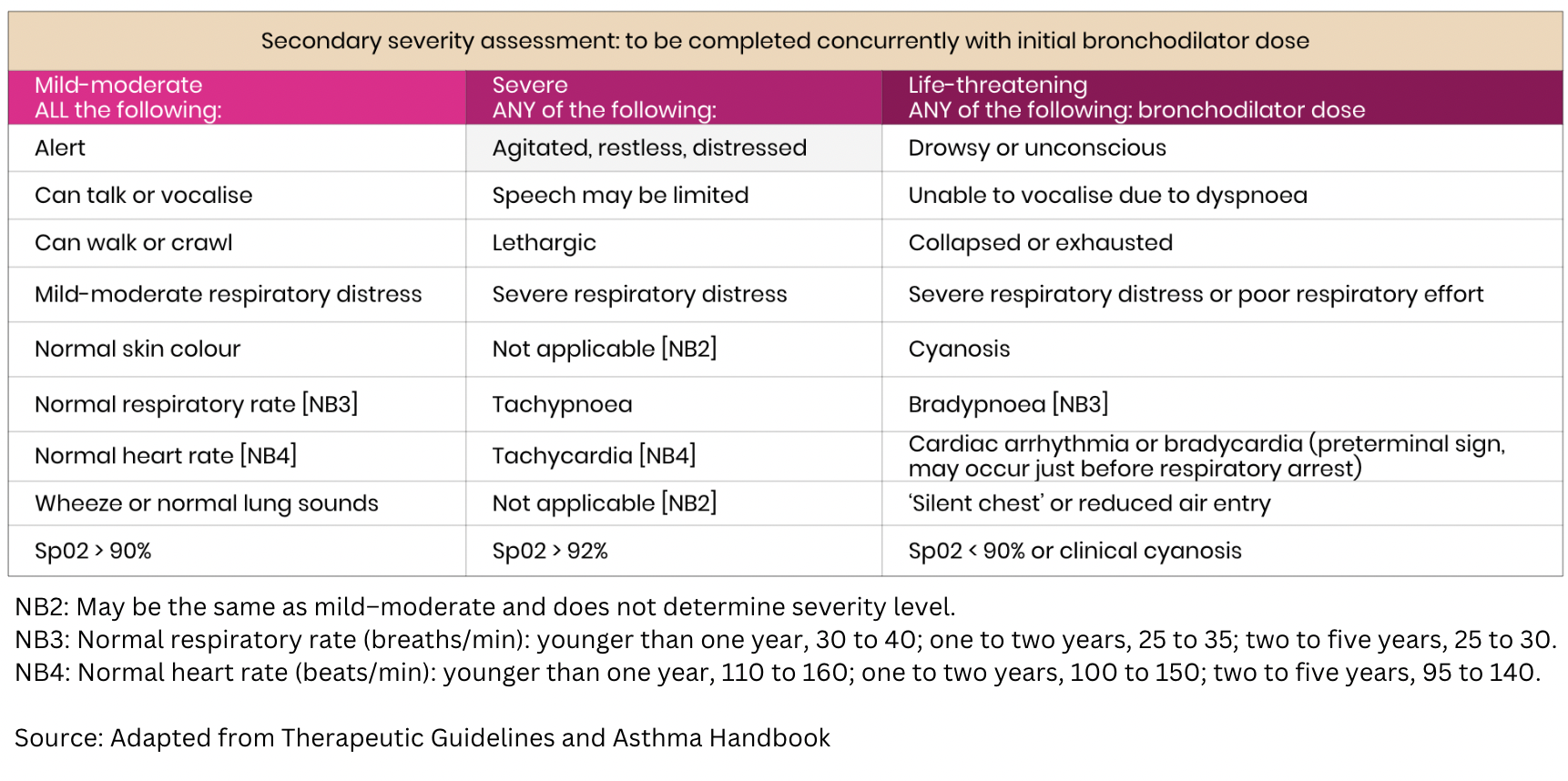
 Secondary severity assessment: to be completed concurrently with initial bronchodilator dose
Secondary severity assessment: to be completed concurrently with initial bronchodilator dose
 Less common causes of respiratory distress in infants
Less common causes of respiratory distress in infants

Investigations for the management of wheeze in pre-school children
 Salbutamol (short acting inhaled beta2 agonist) is recommended for all pre-schoolers with wheeze.
Salbutamol (short acting inhaled beta2 agonist) is recommended for all pre-schoolers with wheeze.
 Ipratropium dosing for the treatment of wheeze in pre-school children
Ipratropium dosing for the treatment of wheeze in pre-school children
 Prednisolone (Oral) dosing for treatment of wheeze in pre-school children
Prednisolone (Oral) dosing for treatment of wheeze in pre-school children
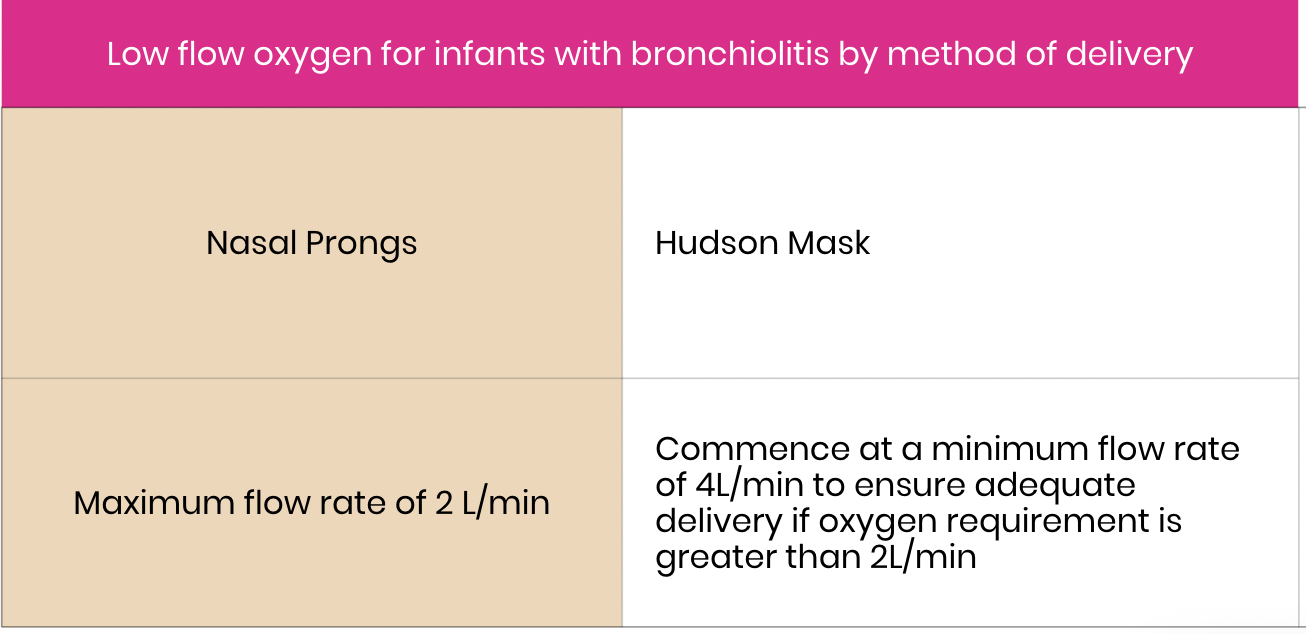
 Low flow oxygen for infants with bronchiolitis by method of delivery
Low flow oxygen for infants with bronchiolitis by method of delivery
{kind=link}
 Magnesium sulphate (IV) dosing for the treatment of wheeze in pre-school children
Magnesium sulphate (IV) dosing for the treatment of wheeze in pre-school children
 Salbutamol (IV) dosing for the treatment of wheeze in pre-school children
Salbutamol (IV) dosing for the treatment of wheeze in pre-school children
 Steroid dosing for the treatment of wheeze in pre-school children
Steroid dosing for the treatment of wheeze in pre-school children
 Oxygen Therapy Flow Chart
Oxygen Therapy Flow Chart
{kind=link}