The main trigger for infant’s respiratory illness and obstructive airway disease is due to a viral infection with little reaction of the smooth muscle of small airways. Therefore, it’s unlikely that small infants react to bronchodilators. However, when infants grow older, and especially children aged 1-4 year develop reactive airways and are more likely to have reactive airways disease (RAD), also known as pre-school wheeze, and hence may respond to bronchodilators.
Children greater than 4 years of age have a more distinct airway reactive pattern of allergies such as allergy pollens (or exercise, cold air). Therefore, a definition of asthma or reactive airway in children aged 1-4 year group is hard to diagnose. In general, it can be said, that in the under 1 year of age group, reactive airways are less likely, and in the 1-4 years we often don’t know and need to test if they respond to bronchodilators. Asthma should be diagnosed preferentially after the age of 4.
Respiratory diseases, particularly the 1–4 year age group have differing diagnosis including bronchiolitis in this age group, which is triggered by a viral illness. The most common disease is Respiratory Syncytial Virus (RSV). Some children can develop less airway disease but more parenchymal disease with infections being either bacterial or viral. Pulmonary parenchyma is a term that refers to the parts of the lungs involved in gas transfer at the alveolar level. These include the alveoli, interstitial tissue, blood vessels, bronchi and bronchioles. These children can present with a classic pneumonia picture, which means certain sections or lobes of lungs, are opacified on a chest x-ray, or they present with a more diffuse pattern of the infection, which is called pneumonitis. Some children can very rapidly develop a bilateral chest infiltrate with a high oxygen requirement and potentially require respiratory support, which is called Acute Respiratory Distress Syndrome (ARDS). Children with ARDS are characterized by widespread inflammation in the lungs. ARDS is not a particular disease, but rather a clinical phenotype (set of observable characteristics of an individual resulting from the interaction of an individual organism within the environment), which may be triggered by various pathologies as outlined, such as pneumonia and sepsis.
A proportion of children present to hospital with an oxygen requirement and airway obstruction/wheeze and can respond quite well to bronchodilators (eg. Salbutamol) and steroids. Some of these cases are triggered by a viral infection, however, can also be triggered by inhaled allergens or other allergies. These children can improve within the first few hours of treatment and are then called RAD.
The overarching description of all these children is acute hypoxaemic respiratory failure (AHRF), which in principle describes these children as having respiratory distress, with increased work of breathing, and an oxygen requirement. For this study, we enrol a large variety of specific individual diseases, however we always target this overarching diagnostic group (AHRF) with High Flow Nasal Cannula (HFNC) therapy treatment, as we are interested in investigating the physiological affect of HFNC therapy and not disease specific response.
To support the breathing with HFNC therapy we must understand that the flow requirement does not increase linearly with weight or growth. The respiratory flow and volume changes during the respiratory cycle follow the growth of the child. After the age of 2-4 years the relative size of the lung and the requirement of respiratory support starts to be more equal to adults, hence the initial 2L/kg/min of support needs to be adapted. Therefore a 20 kg child needs relatively less HFNC rate compared to a 5 kg infant.
The demand for flows when using HFNC follows the length and growth of a normal child. (Note the growth chart in Diagram 4).
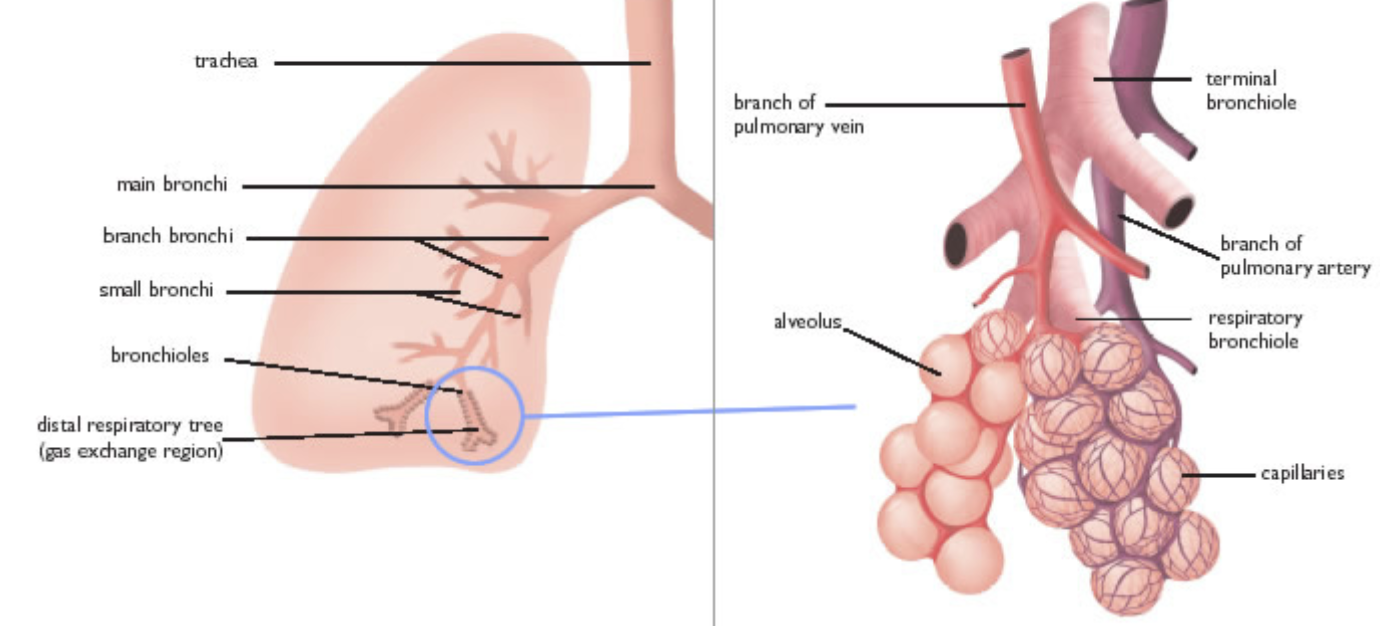
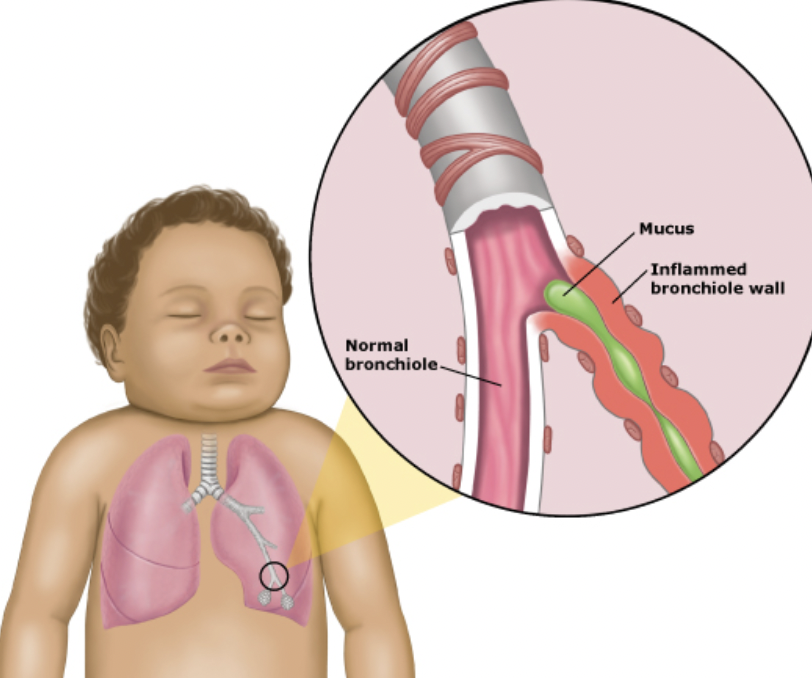
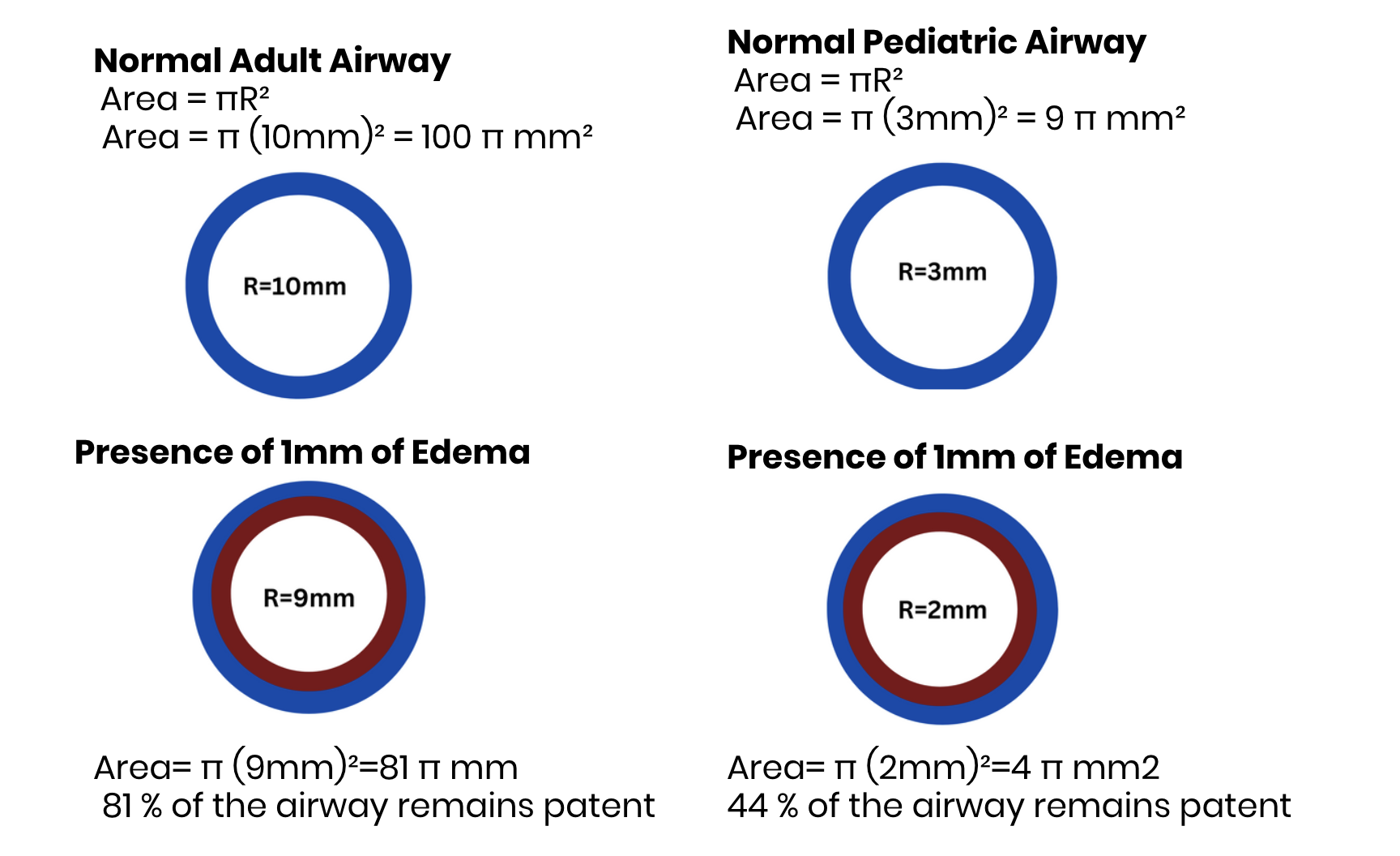
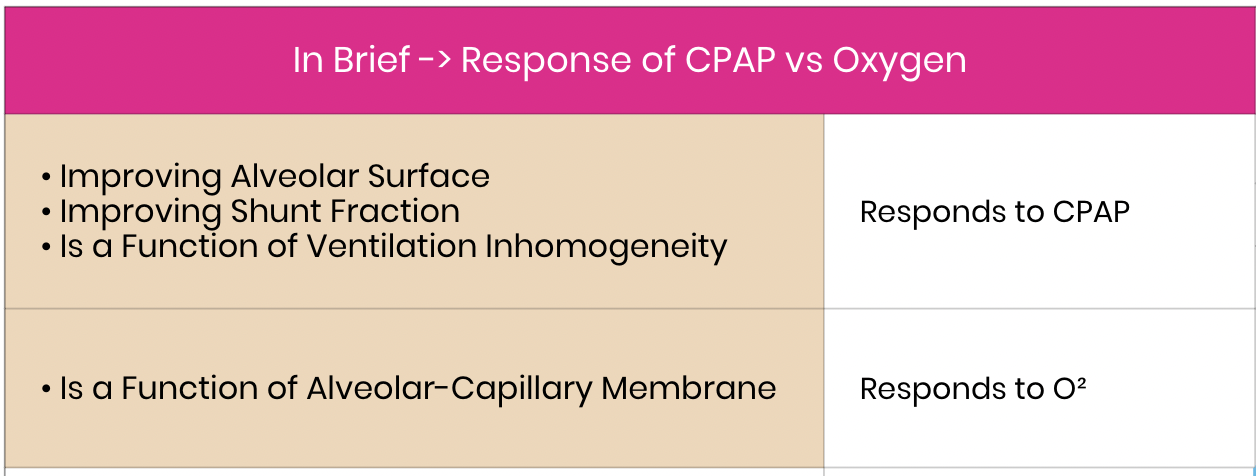
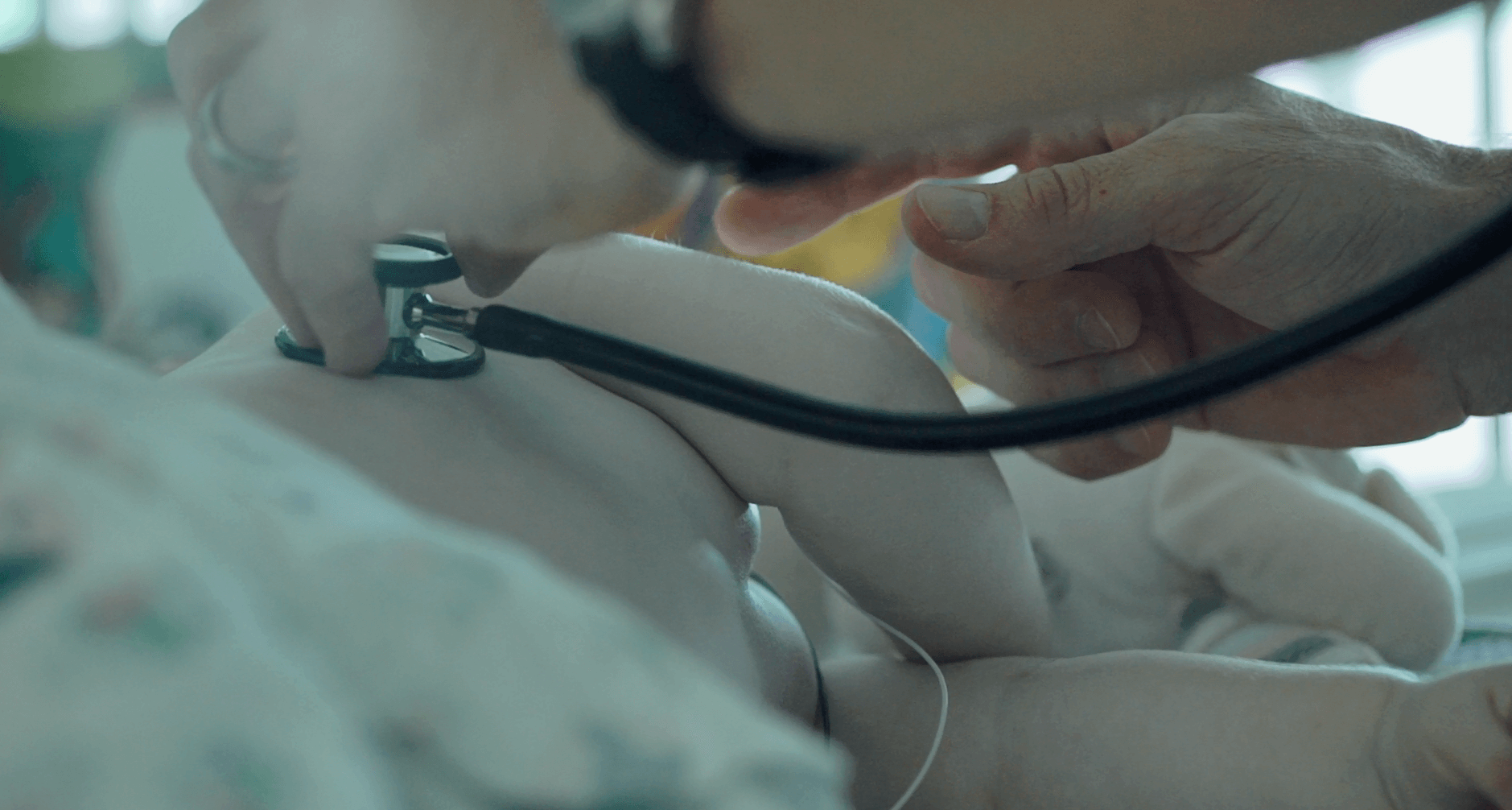
 Diagram 1
Diagram 1 Diagram 2
Diagram 2 Diagram 3
Diagram 3 Diagram 4
Diagram 4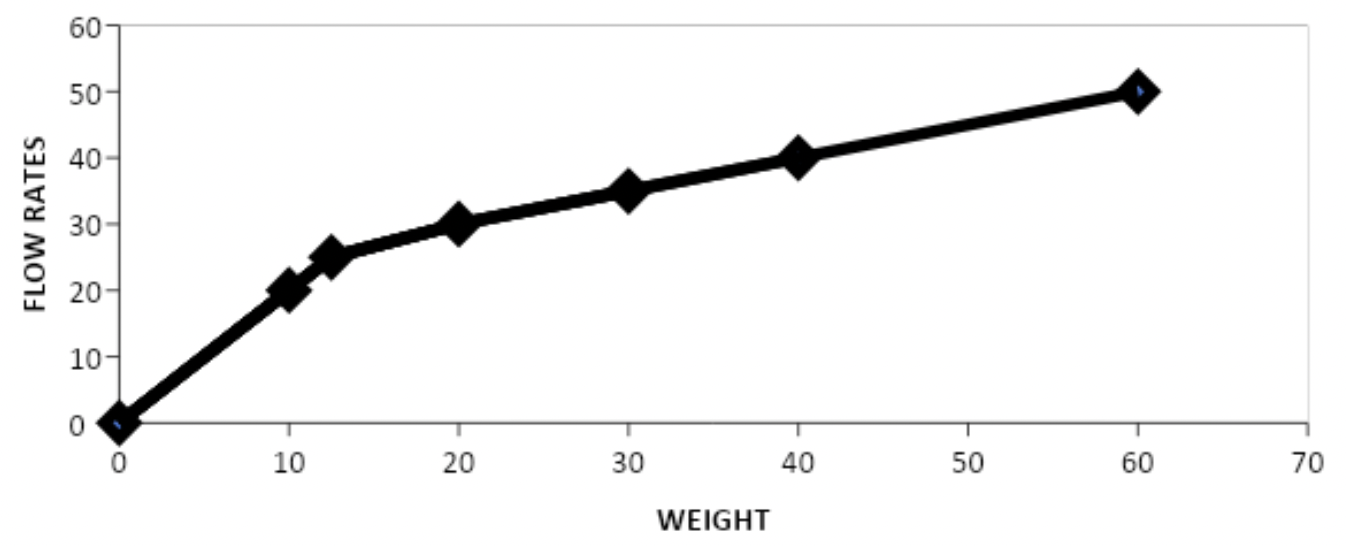{kind=link}