
Community Acquired Pneumonia Treatment Plan Emergency management in children in the remote context
Community-acquired pneumonia is a clinical diagnosis of pneumonia caused by a community-acquired infection in a previously healthy child. Clinical assessment can be challenging; symptoms vary with age and can be non-specific in young children, and aetiology is often unknown at presentation.
Key Points
- A CXR does not need to be routinely performed in children with mild/moderate disease who will be managed as an outpatient if a complication of pneumonia is not clinically suspected.
- High dose oral amoxicillin 30 mg/kg (Maximum 1 g/dose) three times a day is recommended in uncomplicated cases of mild/moderate and severe CAP even if the patient is admitted and if the patient is tolerating oral intake (and not requiring ICU/HDU care).
- In childhood CAP, the benefit of empirical therapy for atypical bacteria is uncertain. In children hospitalised with CAP, add therapy for atypical bacteria only when B.pertussis or M.pneumoniae are clinically suspected.
- Blood and microbiological tests are not recommended as routine investigations in CAP.
- Viruses are the most common cause of CAP in children over 2 months old.
Background
Community acquired pneumonia (CAP) in childhood is an important cause of morbidity in both the developed and developing world. Children with symptoms consistent with CAP present frequently to emergency departments across Queensland. CAP is estimated to have an incidence of 5 to 8 cases per 1000 person years in Australia. The incidence is highest in children less than 5 years old, Indigenous patients and the unimmunised population.
Difficulties with breathing and oxygen requirement as a result of a pneumonia is the most common reason to cause sepsis, hence sepsis and pneumonia should always be considered together.
Assessment
 |
ALERT – Bacterial pneumonia Consider in children when there is persistent or repetitive fever >38.5 degrees Celsius together with chest recession and a raised respiratory rate |
A reasonable definition of pneumonia in childhood may be a persistent or repetitive fever, cough and tachypnoea at rest when clinical wheezing syndromes have been ruled out. It is reasonable to consider pneumonia in any child with fever and tachypnoea if there is not a clear alternate diagnosis. Radiological changes are not required to make the clinical diagnosis as an x-ray is not required in simple pneumonia managed as an outpatient and radiological features can lag behind clinical symptoms.
Community acquired pneumonia is defined as pneumonia occurring in a previously healthy child (or child without respiratory comorbidities) due to an infection acquired outside hospital.
History
History should include capturing specific information on symptoms/signs that could suggest a pneumonia.
These include:
- fever, cough
- Tachypnoea
- increased WOB
- grunting, abdominal pain
- chest pain
- focal or diffuse changes in air entry or crackles/crepitations on chest auscultation, dullness to chest percussion
- new oxygen requirement
There are multiple potential causative organisms in CAP including viruses, bacteria and atypical bacteria. There is no reliable clinical or radiological way to distinguish between these potential causative agents. CAP in children is usually viral, commonly Respiratory syncytial virus (RSV), Adenovirus, Parainfluenza virus, Influenza virus and Human metapneumovirus. The most common bacterial causes are Streptococcus pneumoniae, Staphylococcus aureus and Mycoplasma pneumoniae. Less common pathogens include Chlamydia trachomatis and Bordetella pertussis.
Pneumonia Severity
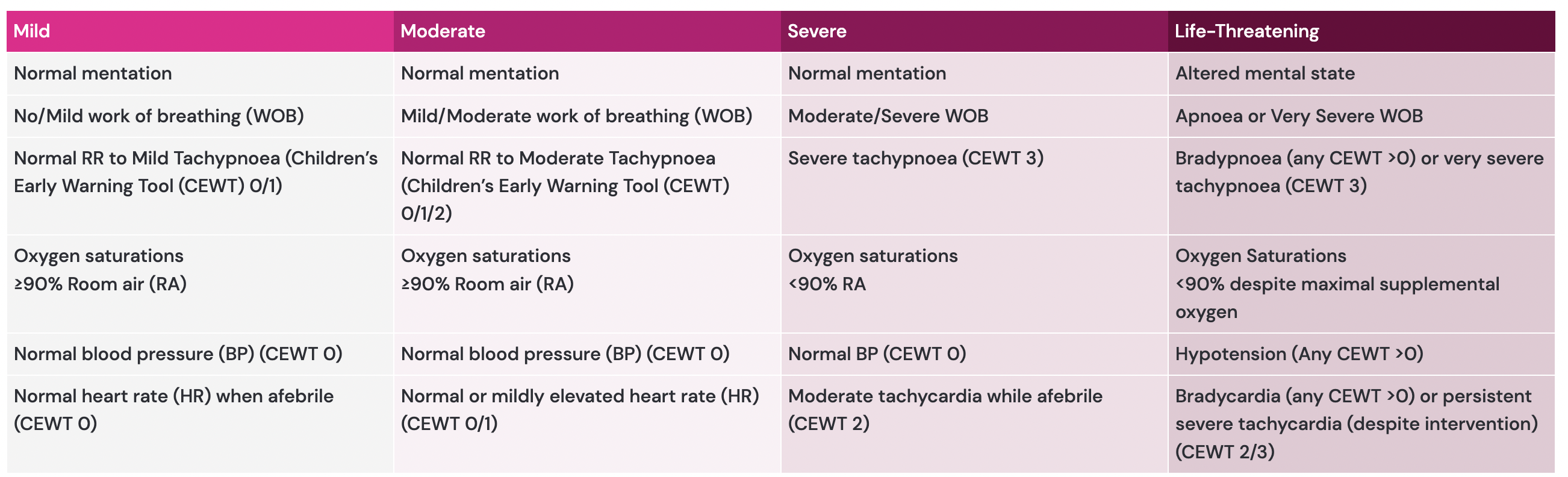
Click image to enlarge
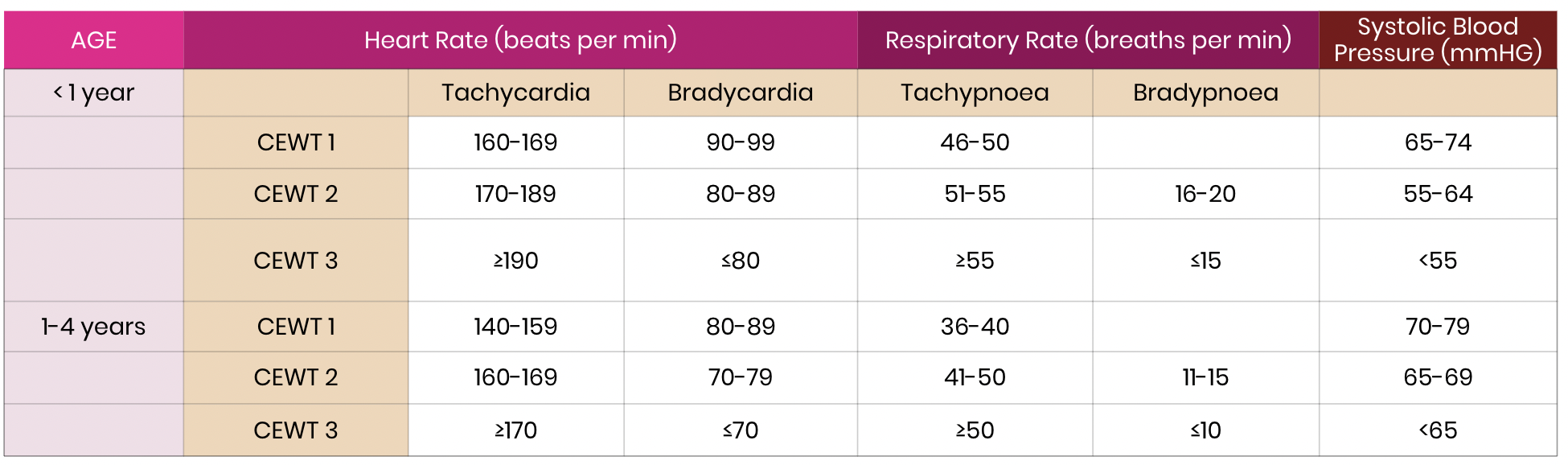
Please see CEWT parameters.
click on table to enlarge

 |
ALERT – Consider seeking senior emergency/paediatric advice as per local protocols for child with severe pneumoniaFive to seven days of total antibiotics is an appropriate duration for most children. Seek senior emergency/paediatric advice as per local protocols for a child with signs of sepsis or persistent hypoxia despite supplemental nasal prong oxygen delivery. Contact paediatric critical care specialist (onsite or via Retrieval Service Queensland (RSQ)) for a child with life-threatening pneumonia or septic shock.(This is also used when specialist teams need to be consulted e.g. Respiratory or Intensive Care Unit (ICU)) |
Management
Investigations
Investigation are not required in children with miild/moderate severity CAP managed as an outpaitent unless there is suspicion of complications.
- A CXR is not required routinely in children with mild/moderate disease managed as an outpatient unless there is a clinical suspicion of a complication. Do not routinely perform lateral x-rays.
- A CXR may be considered for investigation of potential occult pneumonia particularly in the child with fevers of unclear source for >1 day and cough.
- CXR should be performed in severe pneumonia, if there is suspicion for an inhaled foreign body or if there is clinical suspicion for a complication of pneumonia i.e. parapneumonic effusion, empyema, necrotising pneumonia.
The following features increase the risk of empyema
- Age more than 3 years
- Recent varicella infection
- Fever more than 7 days
- Pleuritic chest pain
- Severe CAP
- No response to 48 hours of appropriate antibiotics
- Clinical evidence of effusion – dull to percussion, focally decreased breath sounds, decreased chest expansion
The identification of a causative pathogen for CAP in children is challenging and usually not necessary in an uncomplicated pneumonia outside the HDU/ICU environment.
At present, no blood tests are reliably able to differentiate a viral from a bacterial aetiology in CAP. Blood Pneumococcal PCR can be helpful in severe pneumonia and paired mycoplasma serology (IgM and IgG) and Anti Streptolysin O Titre (ASOT) may provide indirect, usually retrospective, aetiological information. Significantly elevated C-reactive protein levels are suggestive of a bacterial aetiology but should not be interpreted in isolation.
Blood cultures should be taken from any child requiring intravenous therapy.
In older children (older than 5 years), pneumococcal urinary antigen may be informative and should be considered if an aetiological diagnosis is sought.
Investigations that could be considered as an inpatient if an aetiological diagnosis is sought (please see paragraph above for considerations as most children do not require an aetiological diagnosis)
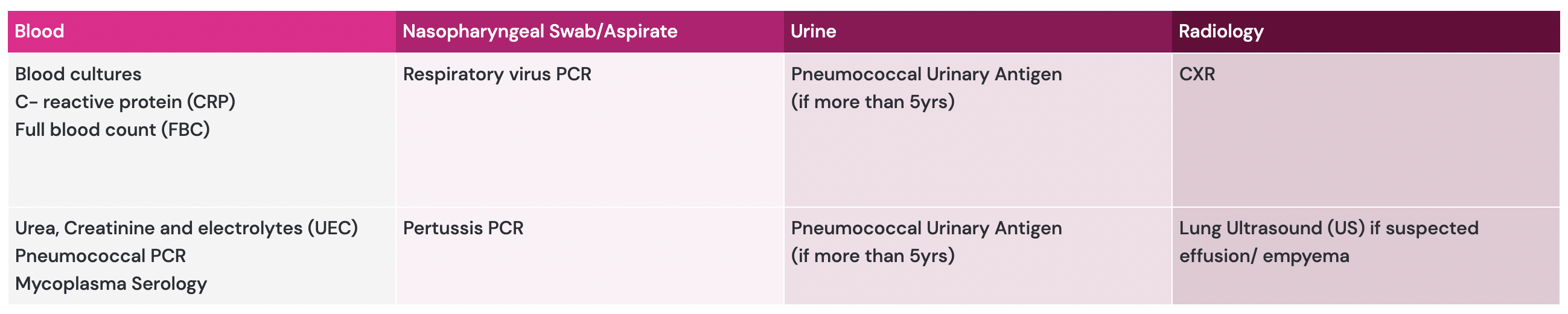
Click on image to enlarge
Treatment
|
ALERT – Oral antibiotics. Oral antibiotics are first-line therapy for children with CAP unless they are unable to tolerate oral antibiotics, have a complication of pneumonia, are septic or require ICU level care |
Five to seven days of total antibiotics is an appropriate duration for most children.
Antibiotics for Community-Acquired Pneumonia (CAP) View Here
Atypical Bacteria
In children hospitalised with CAP, the benefit of empirical therapy for atypical bacteria is uncertain. It is reasonable to add therapy for atypical bacteria to amoxicillin if:
- Bordetella pertussis is suspected (e.g. children who have been in contact with a pertussis case, children with paroxysmal cough associated with cyanosis or apnoea), while awaiting the results of PCR performed on nasopharyngeal samples
- M. pneumoniae is suspected (e.g. school-aged children with rash, children with a household contact who has M. pneumoniae infection, chest pain).
In children with mild to moderate CAP managed as an outpatient it is reasonable to commence amoxicillin alone (without the need for testing) with a plan to add a macrolide (i.e. roxithromycin or azithromycin) if symptoms are not improving after 48 hours (unless Bordetella pertussis is suspected clinically).
ALERT – Empirical therapy for atypical bacteria
In children hospitalised with CAP, the benefit of empirical therapy for atypical bacteria is uncertain and in most cases the addition of macrolide to beta lactam therapy is unnecessary. In hospitalised children it is reasonable to add therapy for atypical bacteria if B. pertussis or M. pneumoniae is suspected.
Children who initially require intravenous therapy should be considered for intravenous to oral switch as soon as there is evidence of clinical improvement, and they are able to tolerate oral therapy. (See CHQ- GDL-01057 Antimicrobial Treatment: Early intravenous to oral switch – Paediatric Guideline).
Five to seven days of total antibiotics is an appropriate duration for most children.
Oxygen Therapy
Apply supplemental oxygen if room air oxygen saturations are below 90%. This can be achieved by a variety of means including nasal prong oxygen, Hudson mask, Humidified High Flow Nasal Cannula. If the patient is requiring an FiO2 of > 40% to maintain oxygen saturations of ≥90% then consider discussion with ICU/RSQ. Consider escalation to invasive respiratory support if altered level of consciousness, recurrent episodes of apnoea, inability to maintain oxygenation despite escalating FiO2 or worsening severe respiratory acidosis.

Other Management
If displaying signs of septic shock manage as Severe Pneumonia with early IV antibiotics and commence sepsis pathway with early IV fluids and early consideration of inotropes. Please see the Sepsis Guideline (CHQ-GDL-60010) for more information.
If there are concerns regarding empyema consult the respiratory team to consider pleural drainage.
Escalation and Advice for Remote Hospitals
For greater detail refer to
- Remote Management of high flow nasal cannula in paediatric patients
- Escalation/Consultation to HFNC for deteriorating patient
Consultation with external paediatric team when:
- Child has specific risk factors (detailed earlier)
- Ongoing hypoxia despite oxygen therapy – Oxygen saturations less than 90% on FiO2 (40%)
- Recurrent apnoeic episodes or slow irregular breathing
- Ongoing haemodynamic shock
- Altered level of consciousness
- Respiratory status assessed as moderate or severe
- Invasive or non-invasive ventilation required
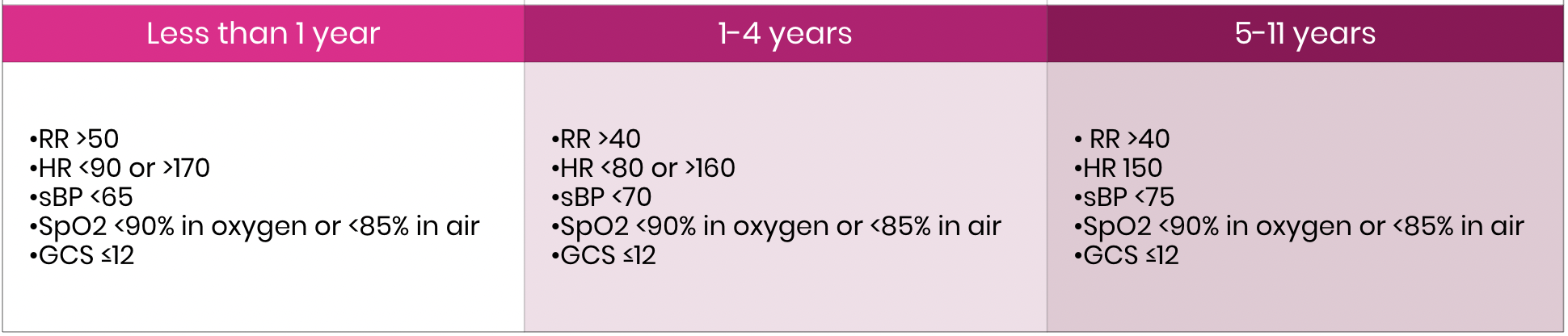
click on image to enlarge
 |
Please ensure the local remote hospitals Senior Medical Officer (or similar) is aware/involved. |
Escalation/Consultation to HFNC therapy for deteriorating patient
HFNC therapy may help avoid intubation but can also provide pre-oxygenation whilst preparation for inevitable intubation is underway.
A randomised controlled study showed that HFNC therapy does not reduce the hospital length of stay but is safe to be used in pre-school wheeze. The outcome of this study suggests that standard oxygen should be the first line oxygen therapy and HFNC only be used if escalation of care is required using the following criteria.
Escalation: Escalation of respiratory support from standard oxygen to HFNC therapy should be considered if one or more of the following is present:
1. heart rate remains >160min for longer than 2 hours
2. respiratory rate remains >45/min for longer than 2 hours
3. oxygen requirement on SOT exceeds standard oxygen therapy (2 L/min by nasal prong, or 8L/min by facemask) to maintain SpO2 ≥90%
4. increased work of breathing requiring escalation of respiratory support and assessed as moderate to severe respiratory failure
Consider transfer to higher level of care if on HFNC and if one or more of the following is present:
1. Heart rate remains >160/min for longer than 2 hours start HFNC
2. Respiratory rate remains >45/min for longer than 2 hours since start of HFNC therapy
3. oxygen requirement on HFNC exceeds FiO2 > 40% (dependant on hospital standard policy) to maintain SpO2 ≥90%
4. The hospital internal Early Warning Tool (CEWT) calls for medical review
For paediatric critical care advice and assistance contact any of the following:
- Level ≥4 CSCF facility consultation MUST be sought within 2 hours of HFNC therapy treatment commencing.
- The level ≥4 CSCF facility to your HHS facility consultation should occur at the Senior Medical Officer (SMO) level from both facilities.
- Referring clinician to contact their relevant level ≥4 CSCF facility for consultation – this should be Senior Medical Officer (SMO) level referral at both facilities.
- If a retrieval is clearly required in the first instance contact RSQ (1 300 799 127) to link all relevant parties together including:
- referring SMO from remote hospital
- local level ≥4 CSCF facility
- relevant local Intensive Care Specialist – dependent on the patient’s condition
- A patient must be accepted at an SMO level at the receiving facility.
- If it is assessed at 2hrs post commencement of HFNC therapy that the patient does not require transfer to a level ≥4 CSCF facility, consultation with the level ≥4 CSCF facility is still mandated to ensure the level ≥4 CSCF facility is aware of the patient and their condition.
- If it is assessed at 2hrs post commencement of HFNC therapy that the patient has not improved or there is further deterioration in their condition, SMO consultation including both level ≥4 CSCF facility and RSQ to arrange retrieval through normal pathways.
These services will provide:
- consultation and access to general paediatric +/- paediatric critical care telephone advice
- coordinate the retrieval of a critically unwell child.
Disposition
Children with CAP could be considered for discharge home if they are mild/moderate in severity, have oxygen saturations ˃90% in room air, are tolerating oral antibiotics and adequate fluids and you have no clinical suspicion of complications or sepsis.
Follow-up
The family should be given a clear management plan in relation to duration of treatment and safety net advice. Specific advice to seek medical review if still febrile or unwell after 48hrs of appropriate oral antibiotics or if child has difficulty breathing.
A routine follow up CXR is not required though it should be considered post round pneumonia, necrotising pneumonia or an empyema.
Consider admission to hospital for:
- Severe pneumonia
- Children not tolerating oral antibiotics
- Children not tolerating adequate oral intake
- Oxygen saturations <90% on RA
- Evidence of complicated pneumonia
- Children with risk factors for deterioration

Diagrams and important tables referenced
 Pneumonia Severity table
Pneumonia Severity table
 CEWT Parameters Table
CEWT Parameters Table
 Investigations Table
Investigations Table

Antibiotics for Community-Acquired Pneumonia
Disclaimer
This guideline is intended as a guide and provided for the PARIS on Country project during the course of the study period. The information has been prepared using a multidisciplinary approach with reference to the best information and evidence available at the time of preparation. This guideline is based of the Children’s Health Queensland Guideline which can be viewed below
The guideline is not a substitute for clinical judgement, knowledge and expertise, or medical advice. Variation from the guideline, taking into account individual circumstances may be appropriate.
This guideline does not address all elements of standard practice and accepts that individual clinicians are responsible for:
- Providing care within the context of locally available resources, expertise, and scope of practice
- Supporting consumer rights and informed decision making in partnership with healthcare
- practitioners including the right to decline intervention or ongoing management
- Advising consumers of their choices in an environment that is culturally appropriate and which enables comfortable and confidential discussion. This includes the use of interpreter services where necessary
- Ensuring informed consent is obtained prior to delivering care
- Meeting all legislative requirements and professional standards
- Applying standard precautions, and additional precautions as necessary, when delivering care
- Documenting all care in accordance with mandatory and local requirements