
Bronchiolitis Respiratory Treatment Plan
Emergency management in children in the remote context
Bronchiolitis is a common lower respiratory tract illness in infants (0-12 months) caused by a viral illness which presents with flu-like symptoms – cough, fever, runny nose. This illness is usually self-limiting within 7-10 days (peaking day 2-3)
Key Points
- Bronchiolitis is a lower viral respiratory tract illness in infants (0-12 months) that is usually self-limiting within 7-10 days (peaking day two to three)
- In most cases, no investigations are required, and treatment is supportive.
- High flow oxygen therapy is recommended for hypoxic bronchiolitis infants (SpO2 <90%).
- Medications such as beta-2-agonists (e.g. salbutamol), corticosteroids, and hypertonic saline are not indicated.
- Refer to the Pre-school Wheeze Guideline for the management of wheeze in children aged 1-5 years.
Background, History, Assessment & Examination
Background
- Bronchiolitis is a clinical diagnosis, based on history and examination.
- Typically begins with an acute upper respiratory tract infection followed by onset of respiratory distress and fever.
- Illness usually resolves without intervention in 7-10 days, with peak severity 2-3 days post onset.
- Cough may persist for weeks.
- Guideline based on the Australasian Bronchiolitis Guideline which has been developed by the Paediatric Research in Emergency Department International Collaborative (PREDICT) research network.
History
History should include specific information on:
- recent respiratory symptoms
- feeding including:
- duration of feeds (feeding more difficult with more severe illness)
- breast feeding
- underlying medical conditions including chronic lung disease,
- congenital heart disease and chronic neurological conditions
- chromosomal abnormalities including Trisomy 21
- Indigenous status
- prematurity
- post-natal exposure to cigarette smoke
Assessment
- A diagnosis of bronchiolitis requires a history of an upper respiratory tract infection followed by onset of respiratory distress with fever and at least one of the following:
- Cough
- Tachypnoea
- Retractions
- Diffuse crackles or wheeze on auscultation
Examination
- Tachypnoea
- Use of Accessory muscles
- Bilateral wheeze and/or fine crepitations
- Hypoxia
Risk Factors for Severe Disease and Differential Diagnosis
Risk Factors
- gestational age less than 37 weeks
- chronological age at presentation less than 10 weeks
- chronic lung disease
- congenital heart disease
- chronic neurological conditions
- Indigenous ethnicity
- failure to thrive
- Trisomy 21
- post-natal exposure to cigarette smoke
- breast fed for less than 2 months
Differential Diagnosis
Whilst bronchiolitis is the most common cause of respiratory distress in infants, less common diagnoses, or dual diagnoses must be considered in all children.
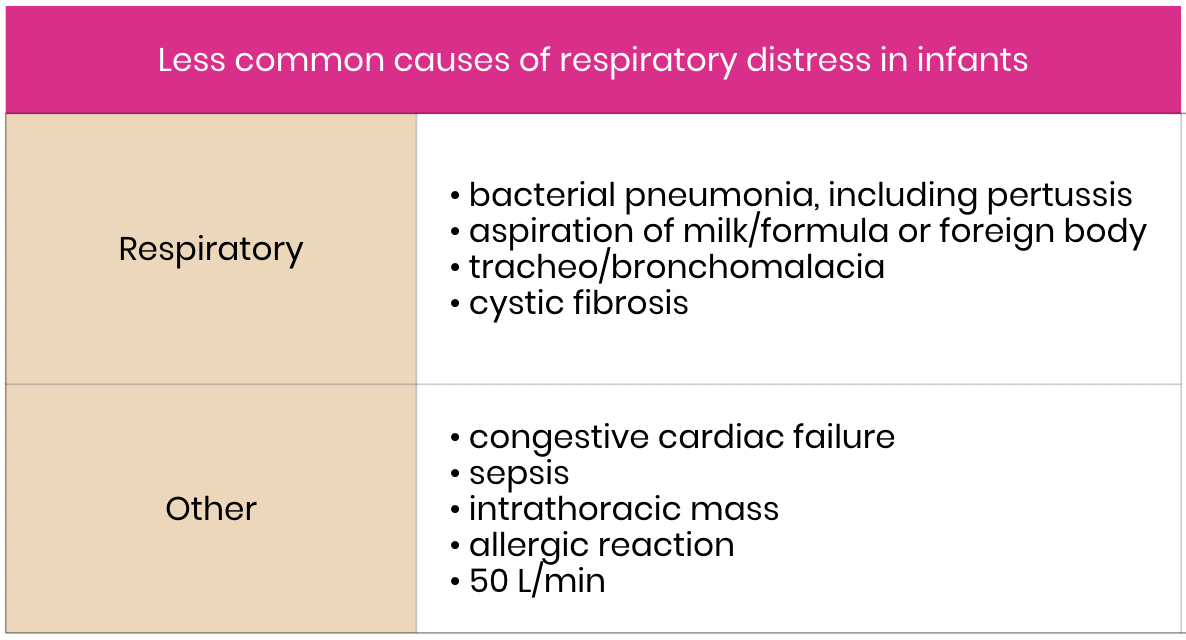
click on table to enlarge
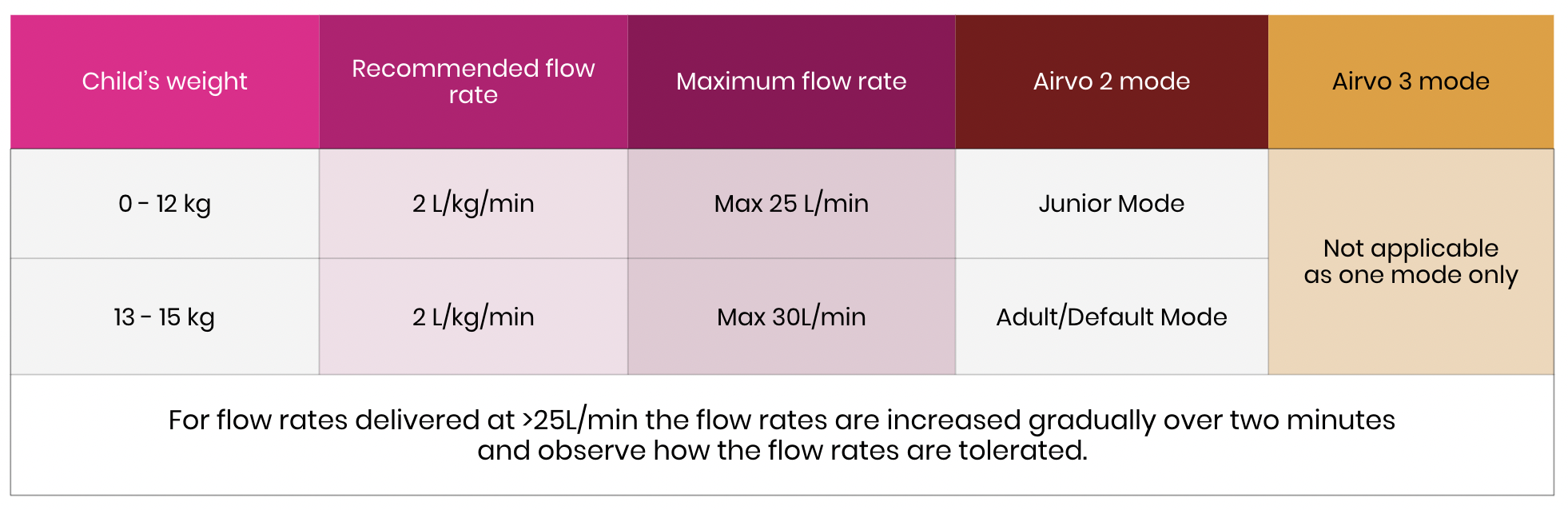
Assessment of severity of acute bronchiolitis
| Mild | Moderate | Severe | |
|---|---|---|---|
| Behaviour | Normal | Some/intermittent irritability | Increasing irritability and/or lethargy/fatigue |
| Respiratory rate | Normal - mild tachypnoea | Increased | Marked increase or decrease |
| Use of accessory muscles | Nil to mild chest wall retraction |
Moderate chest wall retractions Trachael tug Nasal flaring |
Marked chest wall retractions Marked trachael tug Marked nasal flaring |
| Oxygen saturations in room air | Sp02 > 92% | Sp02 90-92% | Sp02 < 90% May not be corrected by 02 |
| Apnoeic episodes | None | May have brief apnoea | May have increasingly frequent or prolonged apnoea |
| Feeding | Normal | May have difficulty with feeding or reduced feeding | Reluctant or unable to feed |

ALERT Consider cardiac disease
In infants with the following:
![]() no precipitating viral illness
no precipitating viral illness
![]() hypoxia out of proportion to severity of respiratory distress
hypoxia out of proportion to severity of respiratory distress
![]() +/- abnormal or unequal peripheral pulses, cardiac murmur or hepatomegaly.
+/- abnormal or unequal peripheral pulses, cardiac murmur or hepatomegaly.
ALERT Congenital cardiac disease
Consider cardiac disease presenting with congestive cardiac failure in infants with no precipitating viral illness, hypoxia out of proportion to severity of respiratory disease and/or presence of abnormal or unequal peripheral pulses, cardiac murmur or hepatomegaly.
ALERT Febrile illness
Children aged less than three months with respiratory symptoms and fever ≥38⁰C may have a concurrent bacterial infection. Refer to Fever Guideline for guidance on investigations and management.
Keep in mind decompensation can be triggered by an intercurrent illness.
Congenital cardiac diseases affect approximately 1% of infants with up to one third diagnosed at over 12 weeks of age. Infants with congestive cardiac failure may present with respiratory distress and decreased feeding. Note that decompensation may be triggered by an intercurrent viral illness.
Management
Investigations
In most children with bronchiolitis, investigations are not routinely required or recommended. Investigations should only be undertaken when there is deterioration or diagnostic uncertainty (eg. cardiac murmur with signs of congestive cardiac failure).
Respiratory viral PCR has no role in the management of individual patients
Chest X-rays (CXR) are not recommenced and may lead to unnecessary antibiotic treatment
Blood tests are not indicated (including blood gas, FBE, blood culture)
Treatment
The primary treatment of bronchiolitis is supportive. This involves ensuring appropriate oxygenation and maintenance of hydration and minimal handling.
 |
Seek URGENT paediatric critical care advice (via Retrieval Services Queensland (advice via Retrieval Services Queensland – RSQ): |
- significant or recurrent apnoeas
- persistent desaturations despite oxygen
- severe disease who are failing to improve with initial treatment
- moderate bronchiolitis with congenital heart disease or chronic lung disease
** Further information can be located in Appendix 1 for a summary of the emergency management for children presenting with symptoms of bronchiolitis.
{kind=link}
Oxygen and respiratory support
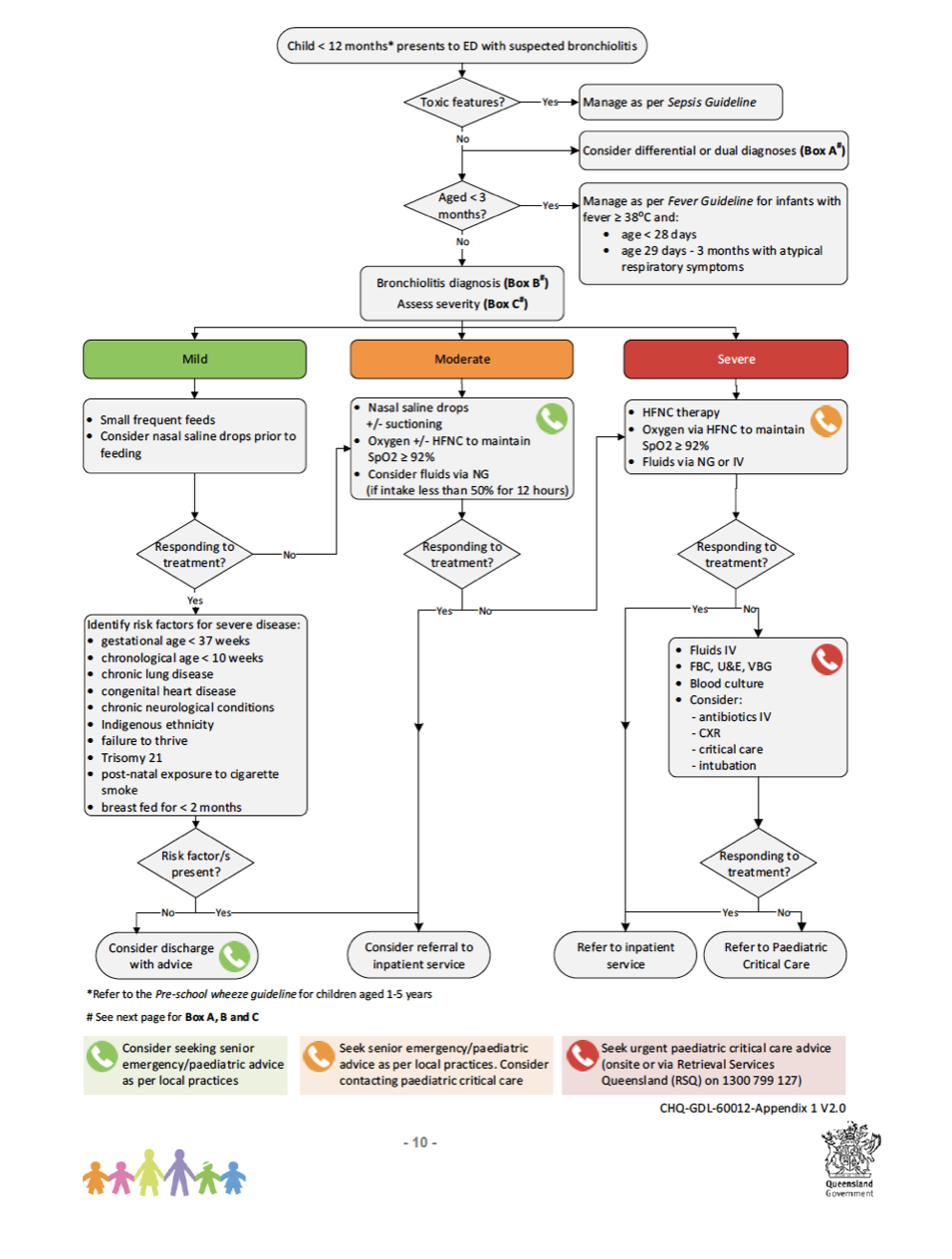
Supplemental Oxygen
- Administer oxygen for children with SpO2 persistently below the target SpO2 (<90%) unless the child has an underlying cardiopulmonary disease with specific SpO2 targets.
- Nasal prong oxygen should only be instituted initially when oxygen saturations are persistently <90%.
- If oxygen saturations remain persistently <90% and there is no improvement in respiratory state despite 2 hours of low flow oxygen, consider high flow nasal cannula oxygen (HFNC) therapy. See Remote Management of high flow nasal cannula in paediatric patients
- Once patient is stable, titrate oxygen down to achieve SpO2 ≥90%. Aim to use minimum supplemental oxygen. It is unnecessary to aim for SpO2 in mid-high 90’s.
- Once no longer requiring supplemental oxygen for 2 hours, discontinue. Continue to monitor observations as required.
click on table to enlarge
High flow nasal cannula oxygen (HFNC) therapy
- Consider HFNC therapy in infants with bronchiolitis who are hypoxic (SpO2 <90%) with moderate to severe work of breathing if a trial of nasal prong oxygen is ineffective.
- Initiation of HFNC therapy must have a plan for ongoing review with a paediatrician or paediatric ICU consultant. See Remote Management of high flow nasal cannula in paediatric patients for all details relating to management in a rural remote hospital including weaning of HFNC.
- HFNC therapy is not recommended for infants without hypoxia.
- Follow local policies and procedures for nursing ratios and ward location.
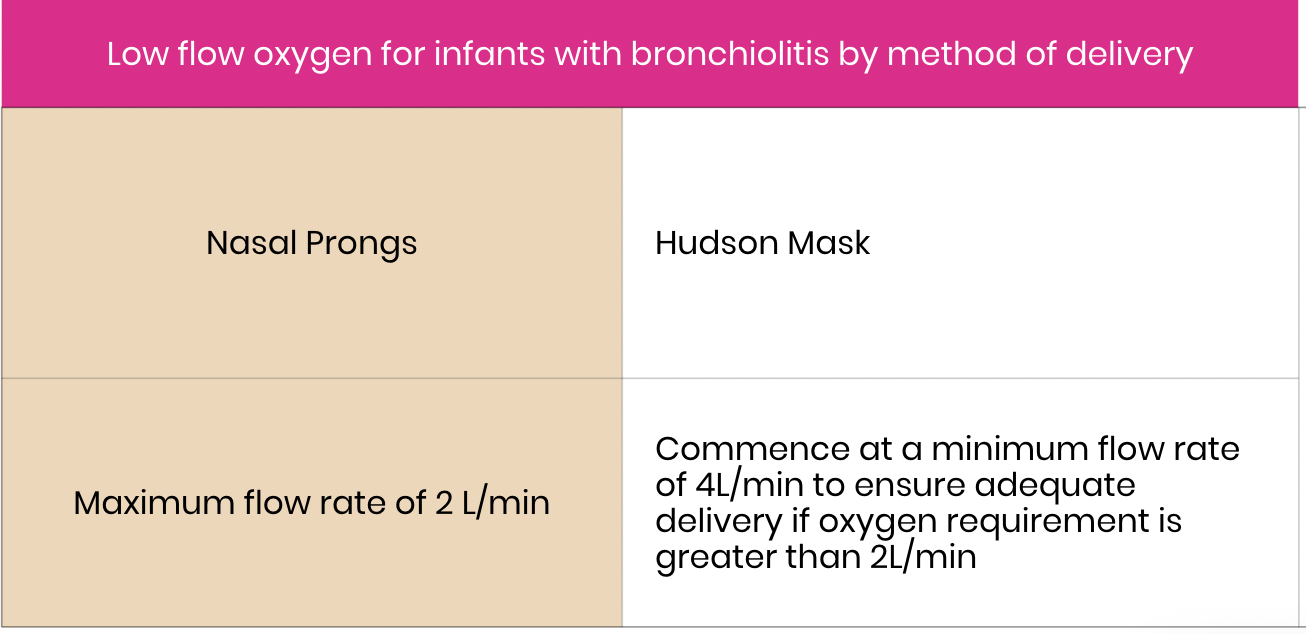
High Flow Nasal Cannula Oxygen Therapy recommended flow rates by weight
Bronchiolitis patients < 12 months
click on diagram to enlarge
Monitoring
Observations should occur in line with local hospital guidelines and Early Warning Tools (EWTs). Continuous pulse oximetry is not routinely recommended for non-hypoxic infants or stable infants receiving oxygen.
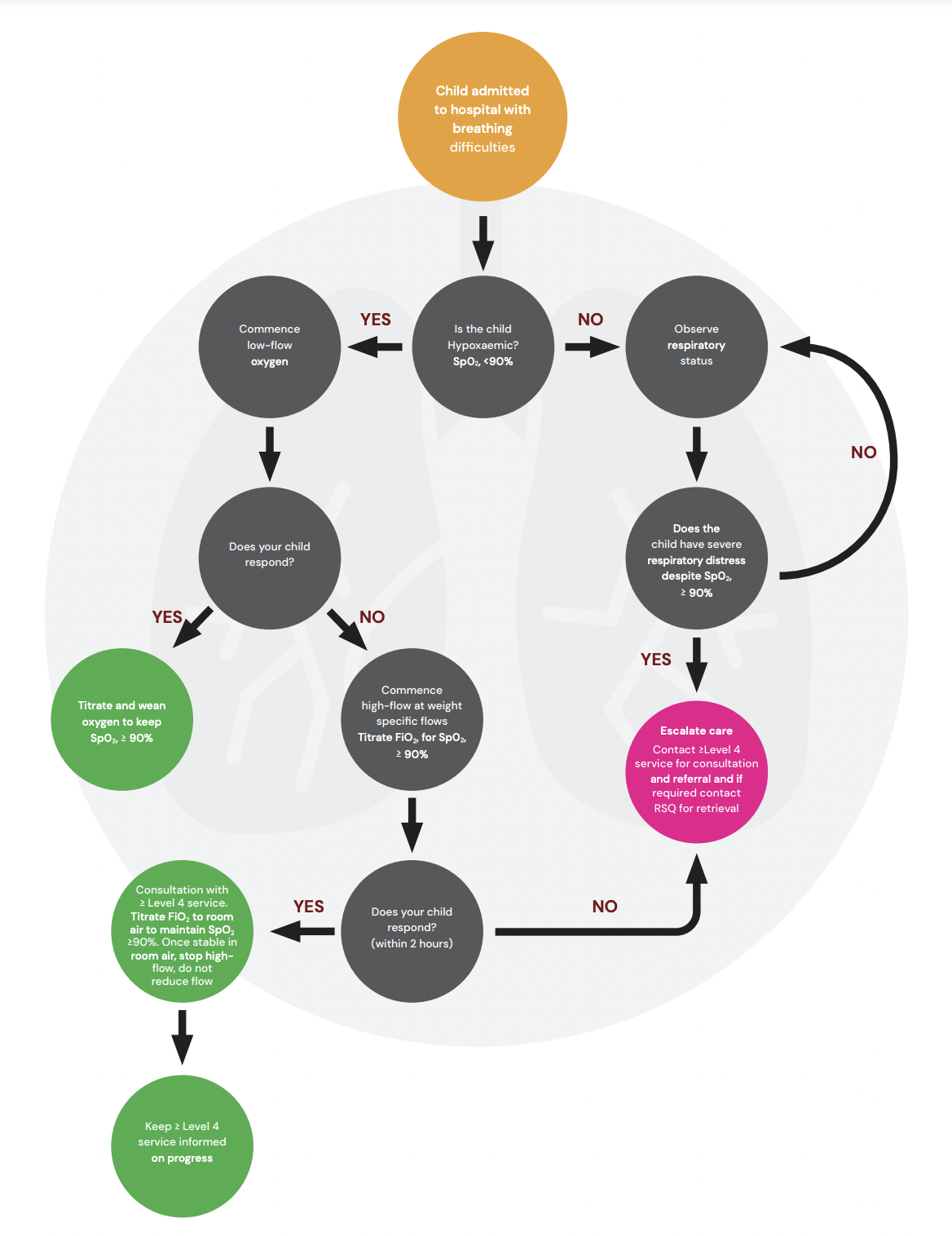
Oxygen Therapy Decision Flow Chart hypoxaemic
 click on the image to enlarge and print
click on the image to enlarge and print
Hydration/Nutrition
- Small frequent feeds are recommended for infants with mild bronchiolitis
- Nasal saline drops may be considered prior to the time of feeding
- Suctioning of the nares may assist feeding in infants with moderate distress
- NGT insertion is highly recommended for infants on HFNC. Advantages include:
- Gastric decompression
- Ability to feed without interrupting HFNC
- Avoid potential for worsening of respiratory symptoms during feeding
- NG or IV hydration is recommended for infants with moderate -severe bronchiolitis who are feeding inadequately (less than 50% over 12 hours)
- If using IV route, isotonic IV fluids (Sodium Chloride 0.9% with glucose, or similar) are recommended
- The volume of fluids required to maintain hydration is unclear
Treatments NOT recommended
- beta 2 agonists (e.g. salbutamol) regardless of a personal/family history of atopy
corticosteroids - adrenaline (nebulised, IM, or IV) except in peri-arrest or arrest situation
- hypertonic saline
- antibiotics
- antivirals
- deep nasal suction
- chest physiotherapy
Nasal Suctioning
Deep suctioning of the nasopharynx is not recommended as may cause oedema and irritation of the upper airway resulting in increased length of illness
Escalation and Advice for Remote Hospitals
For greater detail refer to
- Remote Management of high flow nasal cannula in paediatric patients
- Escalation/Consultation to HFNC for deteriorating patient
 |
Please ensure the local remote hospitals Senior Medical Officer (or similar) is aware/involved. |
Consultation with external paediatric team when:
- child has specific risk factors (detailed earlier)
- ongoing hypoxia despite oxygen therapy
- persistent apnoeic events
- respiratory status assessed as moderate or severe
- physiological triggers including the following as a guide:
- RR >50
- HR <90 or >170
- sBP <65
- SpO2 <90% in oxygen or <85% in air
- GCS ≤12
For paediatric critical care advice and assistance contact any of the following:
- Level ≥4 CSCF facility consultation MUST be sought within 2 hours of HFNC therapy treatment commencing.
- The level ≥4 CSCF facility to your HHS facility consultation should occur at the Senior Medical Officer (SMO) level from both facilities.
- Referring clinician to contact their relevant level ≥4 CSCF facility for consultation – this should be Senior Medical Officer (SMO) level referral at both facilities.
- If a retrieval is clearly required in the first instance contact RSQ (1 300 799 127) to link all relevant parties together including:
- referring SMO from remote hospital
- local level ≥4 CSCF facility
- relevant local Intensive Care Specialist – dependent on the patient’s condition
- A patient must be accepted at an SMO level at the receiving facility.
- If it is assessed at 2hrs post commencement of HFNC therapy that the patient does not require transfer to a level ≥4 CSCF facility, consultation with the level ≥4 CSCF facility is still mandated to ensure the level ≥4 CSCF facility is aware of the patient and their condition.
- If it is assessed at 2hrs post commencement of HFNC therapy that the patient has not improved or there is further deterioration in their condition, SMO consultation including both level ≥4 CSCF facility and RSQ to arrange retrieval through normal pathways
These services will provide:
- consultation and access to general paediatric +/- paediatric critical care telephone advice
- coordinate the retrieval of a critically unwell child.
Disposition
Consider discharge from ED when:
There is insufficient evidence to recommend absolute discharge criteria for infants attending the ED with bronchiolitis.
- Consider discharge for the following infants:
able to maintain adequate oxygen saturations in room air - feeding adequately
- parent/caregiver can safely manage the infant at home (consider time of day, parent/carer comprehension and compliance, access to transport and distance to the local hospital)
Admission for a further period of observation may be considered for infants who meet the above criteria but are early in their illness and have risk factors for more severe disease (refer to Assessment).
On discharge, parent/caregiver should be provided with a Bronchiolitis factsheet and advised to seek medical help prior to next appointment if worsening symptoms and inability to feed adequately.
Follow-up with GP within two to three days or earlier if symptoms worsen.
Consider admission to hospital when:
The decision to admit should be supported by clinical assessment, social and geographical factors and phase of illness.
References
Cunningham et al. Oxygen saturation targets in infants with bronchiolitis (BIDS): a double-blind, randomised, equivalence trial, Lancet 2015; 386: 1041–48.
Franklin et al. A Randomized Trial of High-Flow Oxygen Therapy in Infants with Bronchiolitis. N Engl J Med. 2018 Mar 22;378(12):1121-1131
Diagrams and important tables referenced
 Less common causes of respiratory distress in infants
Less common causes of respiratory distress in infants
 Low flow oxygen with infants with bronchilitis by method of delivery
Low flow oxygen with infants with bronchilitis by method of delivery
 High Flow Nasal Cannula Oxygen Therapy recommended flow rates by weight
High Flow Nasal Cannula Oxygen Therapy recommended flow rates by weight
 Oxygen Therapy Decision Flow Chart hypoxaemic
Oxygen Therapy Decision Flow Chart hypoxaemic
{kind=link}
Disclaimer
This guideline is intended as a guide and provided for the PARIS on Country project during the course of the study period. The information has been prepared using a multidisciplinary approach with reference to the best information and evidence available at the time of preparation. This guideline is based of the Children’s Health Queensland Guideline which can be viewed below
This guideline does not address all elements of standard practice and accepts that individual clinicians are responsible for:
+ Providing care within the context of locally available resources, expertise, and scope of practice
+ Supporting consumer rights and informed decision making in partnership with healthcare practitioners including the right to decline intervention or ongoing management
+ Advising consumers of their choices in an environment that is culturally appropriate and which enables comfortable and confidential discussion. This includes the use of interpreter services where necessary
+ Ensuring informed consent is obtained prior to delivering care
+ Meeting all legislative requirements and professional standards
+ Applying standard precautions, and additional precautions as necessary, when delivering care
+ Documenting all care in accordance with mandatory and local requirements